Doctor-Workers: Unite!
Could Disobedience Be the Path Ahead?
By Howard Waitzkin, M.D., Ph.D.
Medscape, May 20, 2016
"A person can become free through acts of disobedience by learning to say no to power.... At this point in history the capacity to doubt, to criticize and to disobey may be all that stands between a future for mankind and the end of civilization."
- Erich Fromm, On Disobedience1
Disobedience
I confess: I am a disobedient doctor.
After a career in academic medicine and public health, I decided to work part-time in a rural health program. There I began to understand the loss of control over the conditions of medical practice that has affected so many doctors. Administrative demands multiplied and constrained my ability to care for my patients in the ways I thought best.
So I decided to disobey. A seemingly minor training requirement for the International Classification of Diseases, 10th edition (ICD-10), became the administrative demand that pushed me over the line to disobedience. But the struggle might have involved any other segment of clinical medicine, where employer mandates infringe on a doctor's freedom to practice.
Proletarianization
Intrinsically, I have nothing against being a proletarian. I supported much of my education by working as a proletarian—for instance in a tire factory, where I learned first-hand about life as a worker in our capitalist society. Throughout my medical career, I have befriended many "nonprofessional" health workers—wonderful people whose services usually go underappreciated. Such people spend most of their waking lives doing tasks assigned by supervisors, and they enjoy little or no control over the conditions and rhythm of their work.
Medicine, I thought, would provide a way to seize control of my own work process and creativity by organizing at least a large part of the work week as I preferred. A position in academic medicine actually did allow me that liberty, despite the challenges of university bureaucracies—though there, too, autonomy started to erode, a phenomenon usually linked to financial shortfalls and measures of productivity.
However, entering the world of a nonacademic medical employee revealed the awesome scope of proletarianization—a change in doctors' previous social class position. Until the 1980s, doctors for the most part owned or controlled their means of production and conditions of practice. Although their work often was challenging, they could decide their hours of work, the staff members who worked with them, how much time to spend with patients, what to write about their visits in medical records, and how much to charge for their services.
Now the corporations for which doctors work as employees usually control those decisions. Loss of control over the conditions of work has caused much unhappiness in the profession. Early on, an esteemed clinician and mentor described medical proletarianization when it was first emerging as "working on the factory floor."2 Most doctors have become highly paid employees of hospital and health system corporations,3 and around one half of doctors report feeling burned out.4,5 Owing to the mystique of professionalism and their relatively high salaries, doctors often do not realize that their discontent reflects in large part their changing social class position.
Deciding to Disobey
As a doctor-worker, I got into trouble by expressing concerns about the training that our health network (hereafter, referred to as "OHN") was requiring for ICD-10 implementation. Until then, I had received praise and little negative feedback, and had just been reappointed.
OHN had contracted with a corporation (hereafter, "$Corp") to help cope with the transition to ICD-10. This corporation was one of hundreds that have emerged to sell consulting services to healthcare organizations facing the challenges of information technology. Such challenges include electronic health records (EHRs), quality assurance, accountable care, and similar arenas. All involve "metrics" that try to make quality quantifiable, a goal that has generated wide debate.
$Corp's training for ICD-10 took multiple hours of unpaid time, and I decided to disobey the requirement. One reason involved my desire to spend time with a dying friend, which made me even more aware that each moment of life is too precious to waste.
After I previewed the $Corp training, I concluded that its educational quality was poor and that it implicitly encouraged "upcoding," which could generate more payments for OHN. Brief discussions with other practitioners confirmed universal contempt for the training, as well as disgruntled universal compliance. I decided to protest the training.
The Slippery Slope to Fascism
My subsequent interactions with OHN administrators surprised me, despite my knowledge about medical proletarianization. The chief medical information officer (CMIO) at OHN wrote that "Practitioners with incomplete ICD-10 coursework at midnight on 10/7/15 will be suspended until the coursework is completed." In response, I sent an email message asking him to explain the rationale for the training requirement. Copying the chief executive officer (CEO), the CMIO pasted his responses into the text of my original message:
1. Please provide evidence that additional training in ICD-10...improves any measurable patient outcomes, costs, or collections.
Not a debatable point. This is a requirement by OHN, so, sorry to say, whether you agree with it or not, it must be done.
2. Please provide the costs to OHN for the training.
Not relevant, as this is a requirement.
3. Please provide quantitative estimates of the financial benefits of the training for OHN.
Not relevant, as this is a requirement.
4. Please give a concrete description of the process by which you concluded that "completion of this training allows us to achieve both appropriate care and remain fiscally responsible—part of OHN stewardship."
Not relevant, as this is a requirement.
This response pressed one of my alarm buttons, which I might call the "fascism button." In my response, I explained the slippery slope to fascism,6 when people do what they are ordered in their jobs without understanding why. Such unjustified requirements, I argued, deserve our conscientious questioning and sometimes noncompliance.
Standardization
The CMIO was unimpressed with my argument about incipient fascism in the workplace, so I next appealed to practicality. I proposed coming to the office, unpaid, and practicing ICD-10 within our EHR. His reply? "OHN's transformation is a movement to ensure process consistency and standardization.... Therefore, your request for an 'exception' is outside the organization's expectation."
Again, the CMIO's reply pressed an alarm button. I must behave like an automaton in a medical assembly line, "the factory floor" foreseen by my mentor.
I then requested a face-to-face meeting and details about my forthcoming suspension—including, most importantly, a plan of coverage for my patients. I repeated my concerns about authoritarianism in the medical workplace and the extensive evidence that standardization actually may reduce quality, creativity, and productivity.
Punishment
My moral predicament deteriorated quickly. On the next morning, the CEO sent an email message asking for my resignation effective within 1 week, despite packed schedules that included many unstable patients. Then, 5 days before the deadline for suspension, I received a letter stating that my office hours with patients had been canceled until further notice. Because I needed to respond to lab results and urgent messages, I tried to connect with the EHR but found that I had been cut off.
I now faced the apparent abandonment of hundreds of my patients, many of them unstable, who had not received any alternative plan of care. Medical abandonment is unethical according to the American Medical Association Code of Ethics7 and is illegal in many states. I contacted the chief of the medical staff, who got me reconnected to the EHR so that I could manage acute problems for my unstable patients.
Because I was not willing to abandon my patients, I also persuaded an administrator to get me reconnected to the ICD-10 training, which I completed under protest late the next night. On the following morning, a Sunday, I received an email message from the CEO thanking me for completing the training and stating that my breach of contract had been "cured."
Redemption
As a doctor-worker, I faced a challenging ethical situation that included loss of professional autonomy, authoritarian practices in the workplace, and apparent abandonment of patients. My first suspension in more than 40 years of practice also raised concerns, such as: Would a report about the suspension from OHN to the National Practitioner Data Bank affect my medical licenses or ability to practice in other settings? Was it my responsibility to blow the whistle on OHN's practices to licensing, accreditation, and insurance agencies?
My small act of conscientious disobedience eventually led to some unexpected responses. My contract and state law required that OHN convene an external review to examine possible interference with my professional judgment, and the coordinator of the state agency that licenses health facilities expressed willingness to investigate this issue and the abandonment of patients.
Facing the probability of external review, the CEO finally met with me in person, and I proposed a formal mediation process. Instead, the CEO composed a document that included an apology, a statement that information about breach of contract would be removed from my personnel file, a commitment to consider individual physicians' preferences in meeting future training requirements, and a promise to meet individually with a physician when a suspension is considered so that patient care would not be disrupted.
Where is the path toward a noncorporatized vision of what we know medicine can be at its best? I don't think that path involves our continuing acquiescence. I confess that I have decided to approach these problems through personal acts of disobedience. For a person like me, closer to the end of my medical career than the beginning, such acts don't risk much. For others, overcoming the risk will require a more organized approach to disobedience.8 Dare I encourage disobedience in unison? To paraphrase someone else: Doctor-workers of the world, unite!
Dr. Howard Waitzkin is Distinguished Professor Emeritus of Sociology at the University of New Mexico and Adjunct Professor of Internal Medicine at the University of Illinois.
Medscape, May 20, 2016
"A person can become free through acts of disobedience by learning to say no to power.... At this point in history the capacity to doubt, to criticize and to disobey may be all that stands between a future for mankind and the end of civilization."
- Erich Fromm, On Disobedience1
Disobedience
I confess: I am a disobedient doctor.
After a career in academic medicine and public health, I decided to work part-time in a rural health program. There I began to understand the loss of control over the conditions of medical practice that has affected so many doctors. Administrative demands multiplied and constrained my ability to care for my patients in the ways I thought best.
So I decided to disobey. A seemingly minor training requirement for the International Classification of Diseases, 10th edition (ICD-10), became the administrative demand that pushed me over the line to disobedience. But the struggle might have involved any other segment of clinical medicine, where employer mandates infringe on a doctor's freedom to practice.
Proletarianization
Intrinsically, I have nothing against being a proletarian. I supported much of my education by working as a proletarian—for instance in a tire factory, where I learned first-hand about life as a worker in our capitalist society. Throughout my medical career, I have befriended many "nonprofessional" health workers—wonderful people whose services usually go underappreciated. Such people spend most of their waking lives doing tasks assigned by supervisors, and they enjoy little or no control over the conditions and rhythm of their work.
Medicine, I thought, would provide a way to seize control of my own work process and creativity by organizing at least a large part of the work week as I preferred. A position in academic medicine actually did allow me that liberty, despite the challenges of university bureaucracies—though there, too, autonomy started to erode, a phenomenon usually linked to financial shortfalls and measures of productivity.
However, entering the world of a nonacademic medical employee revealed the awesome scope of proletarianization—a change in doctors' previous social class position. Until the 1980s, doctors for the most part owned or controlled their means of production and conditions of practice. Although their work often was challenging, they could decide their hours of work, the staff members who worked with them, how much time to spend with patients, what to write about their visits in medical records, and how much to charge for their services.
Now the corporations for which doctors work as employees usually control those decisions. Loss of control over the conditions of work has caused much unhappiness in the profession. Early on, an esteemed clinician and mentor described medical proletarianization when it was first emerging as "working on the factory floor."2 Most doctors have become highly paid employees of hospital and health system corporations,3 and around one half of doctors report feeling burned out.4,5 Owing to the mystique of professionalism and their relatively high salaries, doctors often do not realize that their discontent reflects in large part their changing social class position.
Deciding to Disobey
As a doctor-worker, I got into trouble by expressing concerns about the training that our health network (hereafter, referred to as "OHN") was requiring for ICD-10 implementation. Until then, I had received praise and little negative feedback, and had just been reappointed.
OHN had contracted with a corporation (hereafter, "$Corp") to help cope with the transition to ICD-10. This corporation was one of hundreds that have emerged to sell consulting services to healthcare organizations facing the challenges of information technology. Such challenges include electronic health records (EHRs), quality assurance, accountable care, and similar arenas. All involve "metrics" that try to make quality quantifiable, a goal that has generated wide debate.
$Corp's training for ICD-10 took multiple hours of unpaid time, and I decided to disobey the requirement. One reason involved my desire to spend time with a dying friend, which made me even more aware that each moment of life is too precious to waste.
After I previewed the $Corp training, I concluded that its educational quality was poor and that it implicitly encouraged "upcoding," which could generate more payments for OHN. Brief discussions with other practitioners confirmed universal contempt for the training, as well as disgruntled universal compliance. I decided to protest the training.
The Slippery Slope to Fascism
My subsequent interactions with OHN administrators surprised me, despite my knowledge about medical proletarianization. The chief medical information officer (CMIO) at OHN wrote that "Practitioners with incomplete ICD-10 coursework at midnight on 10/7/15 will be suspended until the coursework is completed." In response, I sent an email message asking him to explain the rationale for the training requirement. Copying the chief executive officer (CEO), the CMIO pasted his responses into the text of my original message:
1. Please provide evidence that additional training in ICD-10...improves any measurable patient outcomes, costs, or collections.
Not a debatable point. This is a requirement by OHN, so, sorry to say, whether you agree with it or not, it must be done.
2. Please provide the costs to OHN for the training.
Not relevant, as this is a requirement.
3. Please provide quantitative estimates of the financial benefits of the training for OHN.
Not relevant, as this is a requirement.
4. Please give a concrete description of the process by which you concluded that "completion of this training allows us to achieve both appropriate care and remain fiscally responsible—part of OHN stewardship."
Not relevant, as this is a requirement.
This response pressed one of my alarm buttons, which I might call the "fascism button." In my response, I explained the slippery slope to fascism,6 when people do what they are ordered in their jobs without understanding why. Such unjustified requirements, I argued, deserve our conscientious questioning and sometimes noncompliance.
Standardization
The CMIO was unimpressed with my argument about incipient fascism in the workplace, so I next appealed to practicality. I proposed coming to the office, unpaid, and practicing ICD-10 within our EHR. His reply? "OHN's transformation is a movement to ensure process consistency and standardization.... Therefore, your request for an 'exception' is outside the organization's expectation."
Again, the CMIO's reply pressed an alarm button. I must behave like an automaton in a medical assembly line, "the factory floor" foreseen by my mentor.
I then requested a face-to-face meeting and details about my forthcoming suspension—including, most importantly, a plan of coverage for my patients. I repeated my concerns about authoritarianism in the medical workplace and the extensive evidence that standardization actually may reduce quality, creativity, and productivity.
Punishment
My moral predicament deteriorated quickly. On the next morning, the CEO sent an email message asking for my resignation effective within 1 week, despite packed schedules that included many unstable patients. Then, 5 days before the deadline for suspension, I received a letter stating that my office hours with patients had been canceled until further notice. Because I needed to respond to lab results and urgent messages, I tried to connect with the EHR but found that I had been cut off.
I now faced the apparent abandonment of hundreds of my patients, many of them unstable, who had not received any alternative plan of care. Medical abandonment is unethical according to the American Medical Association Code of Ethics7 and is illegal in many states. I contacted the chief of the medical staff, who got me reconnected to the EHR so that I could manage acute problems for my unstable patients.
Because I was not willing to abandon my patients, I also persuaded an administrator to get me reconnected to the ICD-10 training, which I completed under protest late the next night. On the following morning, a Sunday, I received an email message from the CEO thanking me for completing the training and stating that my breach of contract had been "cured."
Redemption
As a doctor-worker, I faced a challenging ethical situation that included loss of professional autonomy, authoritarian practices in the workplace, and apparent abandonment of patients. My first suspension in more than 40 years of practice also raised concerns, such as: Would a report about the suspension from OHN to the National Practitioner Data Bank affect my medical licenses or ability to practice in other settings? Was it my responsibility to blow the whistle on OHN's practices to licensing, accreditation, and insurance agencies?
My small act of conscientious disobedience eventually led to some unexpected responses. My contract and state law required that OHN convene an external review to examine possible interference with my professional judgment, and the coordinator of the state agency that licenses health facilities expressed willingness to investigate this issue and the abandonment of patients.
Facing the probability of external review, the CEO finally met with me in person, and I proposed a formal mediation process. Instead, the CEO composed a document that included an apology, a statement that information about breach of contract would be removed from my personnel file, a commitment to consider individual physicians' preferences in meeting future training requirements, and a promise to meet individually with a physician when a suspension is considered so that patient care would not be disrupted.
Where is the path toward a noncorporatized vision of what we know medicine can be at its best? I don't think that path involves our continuing acquiescence. I confess that I have decided to approach these problems through personal acts of disobedience. For a person like me, closer to the end of my medical career than the beginning, such acts don't risk much. For others, overcoming the risk will require a more organized approach to disobedience.8 Dare I encourage disobedience in unison? To paraphrase someone else: Doctor-workers of the world, unite!
Dr. Howard Waitzkin is Distinguished Professor Emeritus of Sociology at the University of New Mexico and Adjunct Professor of Internal Medicine at the University of Illinois.
Jeffrey Sachs: Bernie Sanders easily wins the policy debate
Jeffrey D. Sachs is director of the Earth Institute and a professor at Columbia University.
Mainstream U.S. economists have criticized Democratic presidential candidate Bernie Sanders’s proposals as unworkable, but these economists betray the status quo bias of their economic models and professional experience. It’s been decades since the United States had a progressive economic strategy, and mainstream economists have forgotten what one can deliver. In fact, Sanders’s recipes are supported by overwhelming evidence — notably from countries that already follow the policies he advocates. On health care, growth and income inequality, Sanders wins the policy debate hands down.
On health care, Sanders’s proposal for a single-payer system has been roundly attacked as too expensive. His campaign (for which I briefly served as a foreign policy adviser) is told that his plan will raise taxes and burst the budget. But this attack misses the whole point of his health proposals. While health spending by the government would go up in the Sanders health plan, private insurance payments would disappear, generating huge net savings for the American people.
Countries such as Canada, Germany, Sweden and Britain all follow something like a single-payer approach and pay much less for health care than the United States does. While the United States spent 16.4 percent of gross domestic product on health care in 2013, Canada paid only 10.2 percent; Germany, 11 percent; Sweden, 11 percent; and Britain, 8.5 percent. U.S. overspending is about 5 percent of GDP, or nearly $1 trillion as of 2016, mainly because of the excessive market power of private health insurers and big drug companies. An authoritative study by the U.S. Institute of Medicine confirms this extent of excess costs, finding losses of about 5 percent of GDP in 2009. Critics of Sanders’s health plan have failed to recognize or acknowledge the huge savings and cost reductions that would accompany a single-payer system.
On economic growth, Sanders also easily wins the debate. While President Obama opted for a short-term stimulus that peaked after two years and disappeared by the end of his first term, and Hillary Clinton has proposed a modest infrastructure program over five years, Sanders calls for a much bolder public investment programdirected at the skills of young people (through free college tuition) and at modernizing and upgrading America’s infrastructure, with a focus on renewable energy, high-speed rail, safe drinking water and urban public transport. Sanders’s growth strategy would get back to fundamentals: a long-overdue increase in productive investments to underpin good jobs and rising worker productivity.
Sanders’s mainstream critics are mostly Keynesians. Their focus is on total spending, whether it’s consumption or investment. Sanders, instead, focuses on investment because long-term growth depends on more rapid capital accumulation (including in skills and technology). America’s slow growth is no mystery. The U.S. net investment rate has declined to about 5 percent of GDP, down from about 10 percent of GDP during the 1960s and 1970s. Sanders’s plan would restore a high-investment economy and, with it, a higher growth rate.
On income distribution, Sanders accurately argues that U.S. income inequality is uniquely high among the rich countries. Only the United States has deep poverty alongside soaring wealth. Only the United States tolerates a hedge-fund industry in which poorly performing money managers (not to mention quite a few crooks) take home billions of dollars in pay, backed by unconscionable tax breaks pushed by Democratic and Republican senators who live off of the largesse of Wall Street.
Consider the most basic measure of income inequality, the Gini coefficient. This measures the inequality of income among households, with zero signifying complete equality and 1 complete inequality. For high-income countries, a Gini coefficient below 0.3 reflects a low degree of income inequality; between 0.3 and 0.4, a moderate degree; and at 0.4 or above, a high degree. According to the most recent data from the Organization for Economic Cooperation and Development, the U.S. Gini coefficient stood at 0.40, with Canada at 0.32; Germany, 0.29; Sweden, 0.27; and Britain, 0.35.
Jeffrey D. Sachs is director of the Earth Institute and a professor at Columbia University.
https://www.washingtonpost.com/opinions/jeffrey-sachs-bernie-sanders-easily-wins-the-policy-debate/2016/05/25/224209a0-21ac-11e6-8690-f14ca9de2972_story.html?hpid=hp_no-name_opinion-card-b%3Ahomepage%2Fstory
Doubling Down on Errors: Urban Institute Defends Its Ridiculously High Single Payer Cost Estimates
by Steffie Woolhandler
Last week we posted a critique of the Urban Institute’s (UI) absurdly biased reportthat claimed Sen. Bernie Sanders’ proposal for single-payer health reform would cause a massive increase in health spending. Now, the report’s authors have issued a 12-page rejoinder to our criticism. But that response is riddled with distortions, misinterpretations and glaring factual errors. Moreover, they now make it clear that they didn’t even try to estimate the costs of Sanders’ (or our) single-payer proposals. Instead, they made up their own reform proposal and costed that out.
Our critique identified three main problems with the UI’s projection that implementing single payer would boost total health spending by $519 billion in 2017. First, UI ignored about 75 percent of the administrative savings that single-payer reform would achieve. Second, it substantially underestimated single payer’s savings on prescription drugs. And finally, it posited an absurdly large increase in the utilization of health care under single payer, far more than could possibly be provided by the current supply of doctors and hospitals.
Below, we briefly discuss the UI’s response to those criticisms, and the facts of the matter.
1. Administrative savings, Part 1: The original UI report projected that single payer could cut insurance overhead from the current 9.5 percent of health spending ($341 billion) to 6 percent ($215 billion). As they now admit, they were modeling a compromised single-payer system, in which private managed care insurers like UnitedHealthcare would continue to play a major role, as they do in the Medicare Advantage program. (Neither we nor Sanders have suggested such a continued role for private insurers.) We pointed out that Canada’s single-payer system runs for 1.8 percent overhead (a figure they impugn, but which is taken directly from Canada’s official health statistics), and is similar to the overhead in the traditional Medicare program. Reducing our insurance overhead to the Canadian level would mean cutting it to “only” $65 billion. There’s no reason to believe we can’t be as efficient as Canada if we, like Canada, proscribe participation by private insurers.
The UI rejoinder argues that “it would be inadvisable to cut administrative costs so much that important functions could not be carried out effectively under a new system. Such functions include rate setting for many different providers of different types facing different costs across the country; quality control over care provision; development, review, and revision of regulations; oversight for fraudulent activity; provider oversight and enforcement of standards; bill payment to providers; consumer services; and more.” Of course traditional Medicare (and Canada) are already doing all of those things, and the UI response gives no reason why $65 billion can’t do the job.
2. Administrative savings, Part 2: The original UI estimate projected that single-payer reform wouldn’t realize any savings on the vast amounts hospitals and doctors currently spend on billing and paperwork. Yet, Sanders’ (and our) proposals would enormously simplify this billing and paperwork. We noted that reliable studies published in the most respected medical and policy journals have documented these provider administrative savings, and that numerous single-payer estimates by the Congressional Budget Office, the Government Accountability Office and private consultants have all assumed that these savings would occur.
In response, our UI colleagues continue to project zero administrative savings for providers, but say: “We agree that administrative costs would fall, but we do not agree they would be close to zero as HW [Himmelstein and Woolhandler] assert.” Actually, we never asserted any such thing. We wrote that “U.S. hospitals spend one-quarter of their total budgets on billing and administration, more than twice as much as hospitals spend in single-payer systems like Canada’s or Scotland’s. Similarly, U.S. physicians, who must bill hundreds of different insurance plans with varying payment and coverage rules, spend two to three times as much as our Canadian colleagues on billing.” Our estimate that cutting U.S. providers’ administrative costs to Canadian levels would save about $2.57 trillion over 10 years was based on this well-established (and peer-reviewed) data.
3. Drug prices: The latest UI piece restated their conviction that a U.S. single-payer system could get only half the discounts that single-payer systems in other nations have gotten from drug companies (and would actually raise drug prices for patients currently on Medicaid). They continue to offer no reason why the discounts would be so small. Moreover, they now claim that Himmelstein and Woolhandler “argue incorrectly that we ignored savings from paying less for prescription drugs.” In fact we didn’t ignore their estimated savings, but said they should be two-fold higher than the 25 percent they projected.
4. Utilization of care, Part 1: The original UI report estimated that single-payer reform would cause a $519 billion increase in health spending in 2017, even accounting for some savings on administration and drugs. But we noted that there just aren’t enough hospital beds or doctors to meet the huge surge in visits and hospitalizations they predict. To back up our claim we cited data from Canada (when its single-payer reform was implemented) and the U.S. (when Medicare and Medicaid were implemented). These data document that no, or very modest increases in society-wide use of care, occurred, and that instead care shifted from the rich and healthy to the sick and poor.
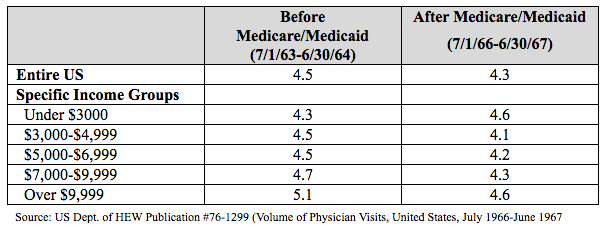
In response, the UI rejoinder says: “Contrary to HW’s [Himmelstein and Woolhandler’s] claim in their article, health care use and spending for the elderly population did increase substantially once the Medicare program was implemented in 1965.” Here (as in their claim about our statement on providers’ administrative costs) they have misquoted us. We wrote that “between 1964 (before Medicare) and 1966 (the year when Medicare was fully functioning) there was absolutely no increase in the total number of doctor visits,” and that “the same thing happened in hospitals.” While we are well aware that utilization by the elderly and the poor went up after Medicare and Medicaid were implemented, the point is that there was a compensatory, slight reduction in utilization by other Americans, reflecting the limitations imposed by the existing supply of hospital beds and doctors (most of whom were already working full time).
Here’s the actual data on the number of doctor visits per person (not just the elderly) before and after Medicare/Medicaid:
And here’s the actual data on the total number of hospitalizations:
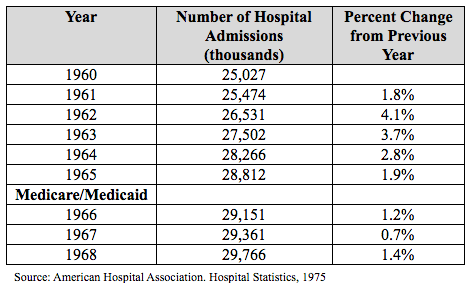
In sum, we were correct in stating that the overall utilization of care showed no surge.
5. Utilization of care, Part 2: We noted in our critique that the lack of a surge in overall utilization in Canada, or with the start-up of Medicare/Medicaid, reflected a shift of care, with the newly insured poor and sick patients getting more of the care they needed, and the healthy and wealthy getting less elective and unnecessary care.
The UI rejoinder disputes that such a shift could occur. “HW [Himmelstein and Woolhandler] indicate that use would increase for the newly insured but would decrease by a similar amount for those already covered as physicians cease unnecessary services for those otherwise covered and perform additional necessary care for those otherwise uninsured. This assumption is faulty for two major reasons. First, no uniform definition of what is necessary and unnecessary exists in medical care; if such a definition existed, insurers would stop paying for all unnecessary care under our current health system. Second, there is absolutely no reason to believe that higher-income, currently insured individuals would lower their use of care under provider supply constraints.”
Their puzzlement displays a lack of familiarity with the considerable literature on variability in the utilization of care between different areas in the U.S., as well as the actual practice of medicine. John Wennberg and colleagues long ago observed that the number of surgical operations in a community showed only modest correlation with needs of the population, but was strongly correlated (r=.64) with the supply of surgeons.
As any doctor knows, doctors play a large role in regulating the amount of care they deliver. If we have no free appointment slots for the next month we’re likely to put off seeing our healthy patients a bit longer. Gastroenterologists often perform unnecessary screening colonoscopies. That’s not something many patients would demand. Indeed, the Aday paper referenced (to support a different point) in the UI rejoinder makes exactly our point: “After Medicare and Medicaid were introduced, providers may have begun to ration the number of visits by the ‘well-to-do’ to accommodate the influx of low-income patients with newly acquired purchasing power and a backlog of unmet need.”
In sum, there’s considerable evidence that doctor routinely adjust the utilization of care by their patients, and that when many additional people gain coverage, doctors shift care to this newly insured group, and compensate by reducing unneeded care for the wealthy and healthy.
6. What system was the UI analyzing? The UI researchers claimed to be estimating the budgetary impact of Sen. Sanders’ proposal. Yet now they tell us, “To be politically acceptable, compromises would have to be made, and those compromises are reflected in our assumptions.” In other words, their estimates are not actually based on the reform that Sanders (or we) have recommended. Instead they assume that the insurance and drug companies are too powerful to really rein in.
Overall, the UI response misrepresents key elements of our critique, and fails to address the erroneous assumptions that underlay their original analysis. Single-payer systems elsewhere provide more and better care at a lower price than we pay. The administrative bloat of our market-driven payment system accounts for much of the difference. While we recognize that a transition to a true single-payer system faces stiff political headwinds, it’s medically and economically feasible. And as Sen. Sanders has shown, political climates can be changed.
Establishment Dems Fight to Defeat 'Medicare-for-All' in Colorado
Pro-Clinton Democrats join Big Pharma and state Republicans in fighting to defeat first-in-the-nation ballot measure for statewide single-payer plan
by Nika Knight - Common Dreams
Highlighting the divisions in the Democratic party this election, Colorado's ballot measure for a universal, single-payer healthcare plan is facing unexpected resistance from the very same party that has been calling for such a healthcare plan since the 1990s.
"There is a disconnect between the powers that be and the people," said state senator Irene Aguilar, a former doctor and the chief architect of the statewide 'Medicare-for-all,' called ColoradoCare, in an interview with the Guardian. "The powers that be are incrementalists. There hasn't been a courage of conviction to try and deal with [healthcare coverage]."
If it passes, ColoradoCare would make Colorado the first state in the nation with universal healthcare.
Most Americans support replacing Obamacare with a single-payer system, and Bernie Sanders has made his support for universal healthcare a central pillar of his presidential campaign. His rival Hillary Clinton, on the other hand, continues to support the least popular position of maintaining the Affordable Care Act (ACA) with only incremental and modest changes.
Clinton's position is echoed by establishment Democrats in Colorado, including Clinton supporter and former governor Bill Ritter, who argued to the Guardian that ColoradoCare was not "practical or feasible."
http://www.commondreams.org/news/2016/05/20/establishment-dems-fight-defeat-medicare-all-colorado
Proposal to Reduce Medicare Drug Payments Is Widely Criticized
by Robert Pear - NYT
An Obama administration proposal to reduce Medicarepayments for many prescription drugs has run into sharp bipartisan criticism, suggesting that it is easier to diagnose the problem of high prices than to solve it.
Patients’ advocates have joined doctors and drug companies in warning that the federal plan could jeopardize access to important medications. Every member of the Senate Finance Committee — 14 Republicans and 12 Democrats — and more than 300 House members have expressed concern.
In a letter to Sylvia Mathews Burwell, the secretary of health and human services, the advocacy arm of the American Cancer Society said the proposal “does not protect cancer patients’ access to the lifesaving drugs needed to treat their disease.” The plan “focuses more on the potential for cost savings” than on how to preserve and enhance the quality of care, it said.
The administration says Medicare’s current payment formula rewards doctors for prescribing expensive drugs. Ms. Burwell has proposed a five-year nationwide test to encourage doctors to prescribe less expensive therapies under Part B of Medicare.
In its proposal, the administration said “we intend to achieve savings,” but did not estimate the amount.
The first phase of the new “payment model” could begin as early Aug. 1. In the second phase, which could start as soon as January 2017, Medicare would link payment to a drug’s value. The government might, for example, pay more for drugs that it deemed more effective in treating or preventing a particular condition. Or it might pay the same amount for drugs that it judged to be “therapeutically similar.”
These drugs — to treat various types of cancer, rheumatoid arthritis, macular degeneration and other conditions — are typically administered in doctors’ offices or hospital clinics. They include drug products that are made from human or animal cells, as well as treatments that mobilize the body’s immune system to fight cancer and other diseases.
Obamacare is still leaving its opponents in pain
by Tom Toles - Washington Post

Doctor Yearns For Return To Time When Physicians Were 'Artisans'
by Michelle Andrews - NPR
In his recent book, The Finest Traditions of My Calling, Dr. Abraham Nussbaum, 41, makes the case that doctors and patients alike are being shortchanged by current medical practices that emphasize population-based standards of care rather than individual patient needs and experiences.
Nussbaum, a psychiatrist, is the chief education officer at Denver Health Medical Center and works on the adult inpatient psychiatric unit there. I recently spoke with him, and this is an edited transcript of our conversation.
Nussbaum, a psychiatrist, is the chief education officer at Denver Health Medical Center and works on the adult inpatient psychiatric unit there. I recently spoke with him, and this is an edited transcript of our conversation.
Your book is in some ways a lament for times gone by, when physicians were "artisans" who had more time for their patients and professional independence. But you're a young doctor and you must have known at the outset that wasn't the way medicine worked anymore. Why do you stick with it?
The first thing I'd say was that I didn't know right away that medicine is no longer universally understood as a calling instead of a job. We are describing health as if it is just another consumer good, and physicians and other health practitioners as the providers of those goods. That is the language of a job. When you remember that being with the ill is a calling, then you remember that it is a tremendous privilege to be a physician. People trust you with their secrets, their fears and their hopes. They allow you to ask about their lives and to assess their bodies. So my lament is not for the loss of physician privilege — goodbye to that — but to the understanding of medicine as a calling.
You don't like checklists and quality improvement measures that dictate how physicians care for patients because you say it turns doctors into technicians and is an obstacle to "moral reasoning." But those tools, which generally take a systems approach to providing care and rely on evidence-based guidelines, aren't going away anytime soon. How do you do the kind of doctoring you want to do in this environment?
The first thing I'd say was that I didn't know right away that medicine is no longer universally understood as a calling instead of a job. We are describing health as if it is just another consumer good, and physicians and other health practitioners as the providers of those goods. That is the language of a job. When you remember that being with the ill is a calling, then you remember that it is a tremendous privilege to be a physician. People trust you with their secrets, their fears and their hopes. They allow you to ask about their lives and to assess their bodies. So my lament is not for the loss of physician privilege — goodbye to that — but to the understanding of medicine as a calling.
You don't like checklists and quality improvement measures that dictate how physicians care for patients because you say it turns doctors into technicians and is an obstacle to "moral reasoning." But those tools, which generally take a systems approach to providing care and rely on evidence-based guidelines, aren't going away anytime soon. How do you do the kind of doctoring you want to do in this environment?
Saving the NHS
Britain’s junior doctors’ strike isn’t just about pay – it’s about preserving a health system based on need, not profit
By Adam Gaffney, M.D.
Jacobin, April 26, 2016
Jacobin, April 26, 2016
Today [April 26] in England, “junior doctors” – post-graduate physicians akin to residents and fellows in the United States – are walking out. This two-day strike represents a major intensification of actions that began in January. It was precipitated by last year’s breakdown in negotiations over a contract that the Conservative government of David Cameron has now proclaimed it will impose come hell or high water. But the stakes of the junior doctors’ strike are much higher.
Physicians’ strikes, it’s worth acknowledging, do not always seek progressive ends. The 1962 Saskatchewan Doctors’ Strike aimed to torpedo the province’s milestone single-payer legislation. But the current action in England, endorsed by a near-unanimous vote last year, is something different. Fundamentally, it’s aimed at the preservation – not the derailment – of universal health care.
The travails of the junior doctors are one part of a much larger campaign. Against austerity, of course. But also for the perseverance of the United Kingdom’s unique health care system – in substance, not merely in name – in the twenty-first century.
A Cracked Foundation
Every nation’s health system is split along a rights-commodity axis, ranging from a public system that provides a universal right to health care according to need, to a private enterprise that profitably provides care according to means. When the National Health Service was founded, notes scholar Rudolf Klein in The New Politics of the NHS, it was the first system that universalized government-provided care, and it thereby skewed health care toward the “rights” side of that axis. As he puts it,
“It [the NHS] was . . . the first comprehensive system to be based . . . on the national provision of services available to everyone. It thus offered free and universal entitlement to State-provided medical care. At the time of its creation it was a unique example of the collectivist provision of health care in a market society.”
In the 1980s, however, Margaret Thatcher’s government began an attack on the principles of the NHS that has not yet subsided. As public health doctor and scholar Allyson Pollock describes in NHS Plc: The Privatisation of our Health Care, Thatcher’s government imposed intermittent austerity funding and the incremental imposition of market-based reforms such as the “internal market” and the “private finance initiative,” signaling a retreat from the NHS’s initial collectivist provisions and a partial move toward commodification.
The Labour government of Tony Blair, as she notes, continued down the road first paved by Thatcher. However, Blair’s government did eventually initiate a much-needed increase in funding: to just under seven percent a year, almost twice the historical average of four percent. This overdue boost, however, would not survive the Great Recession.
In 2010, David Cameron’s Conservative-led government was elected and destabilized the NHS through two great upheavals. First, the government reorganized the NHS through the passage of the 2012 Health and Social Care Act; second, it instituted a period of funding austerity the likes of which the NHS had never seen.
The changes wrought by the 2012 law are complex, and the full ramifications not yet entirely clear. Health policy scholar John Lister described the law in a phone interview as a “massive top-down reorganization of the NHS” that pushes it further onto the free market, effectively displacing (some) care provision into the private sector.
And as Pollock and lawyer Peter Roderick – both supporters and advocates for a fully public NHS – wrote in the British Medical Journal last year, the law calls for a number of “reductions and restrictions [of health care that] pave the way for mixed funding arrangements and a gradual shift to private insurance and charges to patients.”
Essentially, they argue, the law “marked the end of the NHS in England” not only by encouraging further privatization and fragmentation, but by effectively ending the Health Secretary’s legal duty to provide comprehensive health services throughout the nation.
The Scrooge Model
Whether the law will fully undo the NHS or simply prove to be another incremental step remains to be seen. The more immediately harmful trend – and the one largely responsible for the junior doctors’ strike – has been the draconian austerity that the service now faces.
Sorry, We Don’t
Take Obamacare
The growing pains of the health care act are frustrating patients.
by Elisabeth Rosenthal - NYT
MY MOSES and her circle of self-employed small-business owners were supporters of President Obama and the Affordable Care Act. They bought policies on the newly created New York State exchange. But when they called doctors and hospitals in Manhattan to schedule appointments, they were dismayed to be turned away again and again with a common refrain: “We don’t take Obamacare,” the umbrella epithet for the hundreds of plans offered through the president’s signature health legislation.
“Anyone who is on these plans knows it’s a two-tiered system,” said Ms. Moses, describing the emotional sting of those words to a successful entrepreneur.
“Anytime one of us needs a doctor,” she continued, “we send out an alert: ‘Does anyone have anyone on an exchange plan that does mammography or colonoscopy? Who takes our insurance?’ It’s really a problem.”
The goal of the Affordable Care Act, which took effect in 2013, was to provide insurance to tens of millions of uninsured or under-insured Americans, through online state and federal marketplaces offering an array of policies. By many measures, the law has been a success: The number of uninsured Americans has dropped by about half, with 20 million more people gaining coverage. It has also created a host of new policies for self-employed people like Ms. Moses, who previously had insurance but whose old plans were no longer offered.
Yet even as many beneficiaries acknowledge that they might not have insurance today without the law, there remains a strong undercurrent of discontent. Though their insurance cards look the same as everyone else’s — with names like Liberty and Freedom from insurers like Anthem or United Health — the plans are often very different from those provided to most Americans by their employers. Many say they feel as if they have become second-class patients.
Is LePage really such a stalwart opponent of Medicaid expansion?
Gov. Paul LePage is an avowed opponent of Medicaid expansion. But does he really understand the impact of his decision?
We have our doubts after the governor’s Monday appearance on Maine Public Broadcasting Network’s “Maine Calling.” During the hourlong call-in show, the governor demonstrated embarrassingly little understanding of Maine’s health coverage landscape.
Apparently, after signing a state budget early in his tenure as governor to cut back on Medicaid coverage for low-income adults without children, then nixing expansion bills that would restore coverage to that exact population, the governor still thinks Medicaid coverage is an option for childless adults, whose income is 138 percent of the federal poverty level — about $21,300 for a two-person household — or lower.
The governor betrayed his lack of understanding after “Maine Calling” host Jennifer Rooks asked him about health coverage for low-income people caught in Maine’s coverage gap — those who don’t qualify for Medicaid but have incomes too low to qualify for subsidized health insurance through the Affordable Care Act’s online marketplace.
“The state of Maine right now is at 200 percent [of the federal poverty level], which is above what Obamacare says at 138,” LePage replied. “We are providing everything that we can by law. We’re following the law. Expanding Medicaid isn’t going to help those folks, because they don’t qualify anyways. That’s the problem people don’t understand is, they don’t qualify, because we’re already above the 138. We are already paying above 138. We were not allowed to go to 100 percent.”
If that’s actually LePage’s understanding, he has apparently forgotten everything that has happened with Medicaid coverage during his time in office. Here’s a timeline to refresh the governor’s memory:
— When LePage took office, the state’s Medicaid program, MaineCare, offered coverage to parents with dependent children who earned up to 200 percent of the poverty level — about $40,000 for a family of three. Limited coverage was available to adults without children whose income fell below the federal poverty level.
— In 2012, LePage signed a supplemental budget bill that proposed to scale back the coverage threshold for parents to 100 percent of the poverty level and ultimately end coverage for childless adults.
— The problem was, the cuts to parent coverage ran afoul of federal law, specifically a provision of the Affordable Care Act that required that states generally keep their Medicaid programs unchanged until 2014. Ultimately, Maine was allowed to trim parent coverage back to 138 percent of the poverty level, not the 100 percent level sought by the LePage administration. The administration wasn’t allowed to cut off coverage to about 6,000 low-income 19- and 20-year-olds, either — a denial that LePage unsuccessfully attempted to take to the Supreme Court.
— At the start of 2014, the LePage administration was able to lower the coverage threshold to 100 percent of the poverty level for parents. Low-income childless adults also lost their coverage at that time, as Maine’s special arrangement for covering them expired. A Medicaid expansion bill would have spared both populations from coverage cuts, but LePage vetoed expansion legislation.
Today, Maine offers no coverage to low-income adults without children and covers only parents with incomes below the poverty line. But LePage apparently thinks many more Maine residents qualify for Medicaid.
When a listener called in Monday and challenged LePage on his Medicaid misunderstanding, LePage doubled down. The caller said her income was low enough to qualify for Medicaid. Since Maine hadn’t expanded coverage, though, she couldn’t sign up for coverage.
“When I leave here, I’m going to go call the commissioner to see,” LePage said. “There’s something missing here, because that’s the whole purpose. Medicaid are for those below the 138 level, and they get Medicaid.”
Indeed, that’s how the Affordable Care Act was designed — to cover those with the lowest incomes with Medicaid, then subsidize private insurance for those with higher incomes. But since LePage has refused to expand Medicaid, the coverage continuum isn’t working the way he think it’s working.
The exchange got us thinking: Is LePage really such a stalwart opponent of Medicaid expansion, or has he been misunderstanding Medicaid this whole time? It would be shameful if thousands of Mainers were going without health coverage because of LePage’s ignorance.
No comments:
Post a Comment