Why, you may ask, are two articles about the disasterous power grid failure in Tesas included in a blog about Health Care Reform?
It's pretty simple - if you substitute the words "health care" for "energy", "medicare-for-all" for "green revolution", and "COVID-19 pandemic" for climate-change induced freeze" you have a pretty good description of what's happened to our health care system - over-reliance on markets and market-based ideology, almost total abrogation of government responsibility to regulate out-of-control capitalism, and the starving of public sector responsibility (such as investment in public health infrastructure) due to unbridled greed, regardless of the human costs.
And yes, the validity of the shock doctrine as described in Naomi Kleins's essay is still pertinent.
It's an American Malady!
😱
-SPC
Opinion | Why Texas Republicans Fear the Green New Deal
by Naomi Klein - NYT - February 21, 2021
Small government is no match for a crisis born of the state’s twin addictions to market fixes and fossil fuels.
Naomi Klein
Ms. Klein is a senior correspondent at The Intercept and the Gloria Steinem Endowed Chair at Rutgers University. Her new book is “How to Change Everything: The Young Human’s Guide to Protecting the Planet and Each Other.”
Since the power went out in Texas, the state’s most prominent
Republicans have tried to pin the blame for the crisis on, of all
things, a sweeping progressive mobilization
to fight poverty, inequality and climate change. “This shows how the
Green New Deal would be a deadly deal,” Gov. Greg Abbott of Texas said
Wednesday on Fox News. Pointing to snow-covered solar panels, Rick
Perry, a former governor who was later an energy secretary for the Trump
administration, declared in a tweet
“that if we humans want to keep surviving frigid winters, we are going
to have to keep burning natural gas — and lots of it — for decades to
come.”
The claims are outlandish. The Green New Deal is, among
other things, a plan to tightly regulate and upgrade the energy system
so the United States gets 100 percent of its electricity from renewables
in a decade. Texas, of course, still gets the majority of its energy from gas and coal; much of that industry’s poorly insulated infrastructure froze up
last week when it collided with wild weather that prompted a huge surge
in demand. (Despite the claims of many conservatives, renewable energy
was not to blame.)
It was the very sort of freakish weather system now increasingly
common, thanks to the unearthing and burning of fossil fuels like coal
and gas. While the link between global warming and rare cold fronts like
the one that just slammed Texas remains an area of active research, Katharine Hayhoe, a climate scientist at Texas Tech University, says the increasing frequency of such events should be “a wake up call.”
But
weather alone did not cause this crisis. Texans are living through the
collapse of a 40-year experiment in free-market fundamentalism, one that
has also stood in the way of effective climate action. Fortunately,
there’s a way out — and that’s precisely what Republican politicians in
the state most fear.
An Energy-Market Free-for-All
A fateful series of decisions were made in the late-’90s, when the now-defunct, scandal-plagued energy company Enron led a successful push
to radically deregulate Texas’s electricity sector. As a result,
decisions about the generation and distribution of power were stripped
from regulators and, in effect, handed over to private energy companies.
Unsurprisingly, these companies prioritized short-term profit over
costly investments to maintain the grid and build in redundancies for
extreme weather.
Today, Texans are at the mercy of regulation-allergic politicians who failed to require that energy companies plan for shocks or weatherize their infrastructure (renewables and fossil fuel alike). In a recent appearance on
NBC’s “Today” show, Austin’s mayor, Steve Adler, summed it up: “We have
a deregulated power system in the state and it does not work, because
it does not build in the incentives in order to protect people.”
This energy-market free-for-all means that as the snow finally
melts, many Texans are discovering that they owe their private
electricity providers thousands of dollars — a consequence of leaving
pricing to the whims of the market. The $200,000 energy bills some people received, the photos of which went viral online, were, it seems, a mistake. But some bills approaching $10,000
are the result of simple supply and demand in a radically
underregulated market. “The last thing an awful lot of people need right
now is a higher electric bill,” said
Matt Schulz, chief industry analyst with LendingTree. “And that’s
unfortunately something a lot of people will get stuck with.” This is
bad news for those customers, but great news for shale gas companies
like Comstock Resources Inc. On an earnings call last Wednesday, its
chief financial officer said, “This week is like hitting the jackpot with some of these incredible prices.”
Put
bluntly, Texas is about as far from having a Green New Deal as any
place on earth. So why have Republicans seized it as their scapegoat of
choice?
A Shock to the System
Blame
right-wing panic. For decades, the Republicans have met every disaster
with a credo I have described as “the shock doctrine.” When disaster
strikes, people are frightened and dislocated. They focus on handling
the emergencies of daily life, like boiling snow for drinking water.
They have less time to engage in politics and a reduced capacity to
protect their rights. They often regress, deferring to strong and
decisive leaders — think of New York’s ill-fated love affairs with
then-Mayor Rudy Giuliani after the 9/11 attacks and Gov. Andrew Cuomo in
the early months of the Covid-19 pandemic.
Large-scale shocks — natural disasters, economic collapse, terrorist attacks — become ideal moments to smuggle in unpopular free-market policies
that tend to enrich elites at everyone else’s expense. Crucially, the
shock doctrine is not about solving underlying drivers of crises: It’s
about exploiting those crises to ram through your wish list even if it
exacerbates the crisis.
To explain this phenomenon, I often quote a guru of the free market revolution, the late economist Milton Friedman. In 1982, he wrote
about what he saw as the mission of right-wing economists like him:
“Only a crisis — actual or perceived — produces real change. When that
crisis occurs, the actions that are taken depend on the ideas that are
lying around. That, I believe, is our basic function: to develop
alternatives to existing policies, to keep them alive and available
until the politically impossible becomes politically inevitable.”
Republicans
have effectively deployed this tactic even after crises like the 2008
market collapse, created by financial deregulation and made deadlier by
decades of austerity. Democrats have, largely, been willing partners.
This seems counterintuitive, but it all comes back to Friedman’s credo:
The change doesn’t depend on the reasons for the crisis, only on who has
the ideas “lying around” — a kind of intellectual disaster
preparedness. And for a long time, it was only the right, bolstered by a
network of free-market think tanks linked to both major parties, that
had its ideas at the ready.
When Hurricane Katrina broke through
New Orleans’s long-neglected levees in 2005, there was, briefly, some
hope that the catastrophe might serve as a kind of wake-up call.
Witnessing the abandonment of thousands of residents on their rooftops
and in the Superdome, small-government fetishists suddenly lost their
religion. “When a city is sinking into the sea and rioting runs rampant,
government probably should saddle-up,” Jonah Goldberg, a prominent
right-wing commentator, wrote at the time. In environmental circles, there was also discussion that the disaster could spur climate action. Some dared to predict
that the collapsed levees would be for the small-government,
free-market legacy of Reaganism what the fall of the Berlin Wall was for
Soviet Communism.
None of it happened. Instead, New Orleans
became a laboratory for the shock doctrine. Public schools were shut
down en masse, replaced by charter schools. Public housing was
demolished, and costly townhouses sprang up, preventing thousands of the
city’s poorest residents, the majority of them Black, from ever
returning. The reconstruction of the city became a feeding ground for
private contractors. Republicans used the cover of crisis to call for
expanded oil and gas exploration and new refinery capacity, much as Mr.
Perry is doing right now in Texas with his calls for doubling down on
gas.
Many tried to stop them. Teachers’ unions, despite having
their members scattered throughout the country, did their best to fight
the privatizations. Residents of public housing and their supporters faced tear gas
to try to stop the demolition of their homes. But there were no readily
available, alternate ideas lying around for how New Orleans could be
rebuilt to make it both greener and fairer for all of its residents.
Even
if there had been, there was no political muscle to turn such ideas
into reality. Though the environmental justice movement has deep roots
in Louisiana’s “cancer alley,” the climate justice movement
was only just emerging at the time Katrina struck. There was no Sunrise
Movement, the youth-led organization that occupied Nancy Pelosi’s
office after the 2018 midterms to demand
“good jobs, and a livable planet.” There was no “squad,” the ad hoc
alliance of congressional progressives whose most visible member,
Alexandria Ocasio-Cortez, sent shock waves through Washington by joining
the Sunrisers in their occupation. There had not yet been two Bernie
Sanders presidential campaigns to show Americans how popular these ideas really are. And there was certainly no national movement for a Green New Deal.
Lying in Ruin
The
difference between then and now goes a very long way toward explaining
why Mr. Abbott is railing against a policy plan that, as of now, exists
primarily on paper. In a crisis, ideas matter — he knows this. He also
knows that the Green New Deal, which promises to create millions of
union jobs building out shock-resilient green energy infrastructure,
transit and affordable housing, is extremely appealing. This is
especially true now, as so many Texans suffer under the overlapping
crises of unemployment, houselessness, racial injustice, crumbling
public services and extreme weather.
All that Texas’s Republicans
have to offer, in contrast, is continued oil and gas dependence —
driving more climate disruption — alongside more privatizations and cuts
to public services to pay for their state’s mess, which we can expect
them to push in the weeks and months ahead.
Will it work? Unlike
when the Republican Party began deploying the shock doctrine, its
free-market playbook is no longer novel. It has been tried and
repeatedly tested: by the pandemic, by spiraling hunger and joblessness,
by extreme weather. And it is failing all of those tests — so much so
that even the most ardent cheerleaders of deregulation now point to
Texas’s energy grid as a cautionary tale. A recent article in the Wall Street Journal, for instance, called the deregulation of Texas’s energy system “a fundamental flaw.”
In
short, Republican ideas are no longer lying around — they are lying in
ruin. Small government is simply no match for this era of big,
interlocking problems. Moreover, for the first time since Margaret
Thatcher, Britain’s former prime minister, declared
that “there is no alternative” to leaving our fates to the market,
progressives are ready with a host of problem-solving plans. The big
question is whether the Democrats who hold power in Washington will have
the courage to implement them.
The horrors currently unfolding in
Texas expose both the reality of the climate crisis and the extreme
vulnerability of fossil fuel infrastructure in the face of that crisis.
So of course the Green New Deal finds itself under fierce attack.
Because for the first time in a long time, Republicans face the very
thing that they claim to revere but never actually wanted: competition —
in the battle of ideas.
There is a great deal of nonsense
being written and spoken about this week’s power failures in Texas,
which left a number of people dead and millions without power or potable
water, sometimes for days.
Among the more prominent nonsense peddlers was the Texas governor, Greg Abbott, who blamed the mess
on wind power and other renewable fuels, while warning that proposals
like the Green New Deal — which would zero out fossil fuels — would more
or less be the end of civilization as we know it. There was also Rick
Perry, the state’s former governor, who seemed to suggest that using
more renewables would lead to socialism, and Representative Dan
Crenshaw, who blamed the whole thing on that liberal bastion otherwise
known as California. “Bottom line,” Mr. Crenshaw wrote on Twitter, “Texas’s biggest mistake was learning too many renewable energy lessons from California.”
These
statements were catnip to progressives, who mainly blamed the state’s
libertarian energy system, which, they claimed, sought to keep prices
low at the expense of safety.
None of the poppycock from Texas
politicians is of any help to the scores of Texans who spent long hours
and days freezing in their homes. It has also obscured the real reasons
for the disaster and diverted attention from an important lesson: that
the nation’s energy delivery system, not just in Texas but everywhere,
needs a radical overhaul if it is to withstand future shocks and play
the role that President Biden has assigned it in the battle against
climate change.
Both sides have elided an interesting
piece of Texas history. The person who put wind power on the Texas map
was a Republican named George W. Bush. As governor, in 1999, Mr. Bush
signed a law deregulating the state’s power market, at which point Texas
started building loads of wind turbines. Wind now supplies about a
quarter of the state’s energy diet — natural gas is about twice that —
and Texas is far and away the biggest supplier of wind energy in the
country and among the biggest in the world.
But wind, which
supplies a smaller fraction of power in wintertime, had little to do
with this week’s disaster. The simple truth is that the state was not
prepared for the Arctic blast. A few wind turbines froze up, but the
main culprits were uninsulated power plants run by natural gas. In
northern states, such plants are built indoors; in Texas, as in other
Southern states, the boilers and turbines are left exposed to the
elements.
There are two lessons here to be absorbed and acted on.
First, the country’s energy systems must be robust enough to withstand
whatever surprises climate change is likely to bring. There is little
doubt that a warming climate turned California’s forests into
tinderboxes, leading to last summer’s frightening wildfires. The
scientific connection between climate change and extreme cold is not as
well established, but it would be foolish to assume that it is not
there. (The dominant hypothesis is that global warming has weakened the
air currents that keep the polar vortex and its freezing winds in
check.) As the Princeton energy expert Jesse Jenkins observes in a recent Times Op-Ed,
we know that climate change increases the frequency of extreme heat
waves, droughts, wildfires, heavy rains and coastal flooding. We also
know the damage these events can cause. To this list we should now add
deep freezes.
If building resilience is one imperative, another is
making sure that America’s power systems, the grid in particular, are
reconfigured to do the ambitious job Mr. Biden has in mind for them — to
not just survive the effects of climate change but to lead the fight
against it. Mr. Biden’s lofty goal is to achieve net zero greenhouse gas
emissions by midcentury and to eliminate fossil fuel emissions from the
power sector by 2035. In the simplest terms, this will mean
electrifying everything in sight: a huge increase in battery-powered
cars and in charging stations to serve them; a big jump in the number of
homes and buildings heated by electric heat pumps instead of oil and
gas; and, crucially, a grid that delivers all this electricity from
clean energy sources like wind and solar.
This, in
turn, will require from Congress a cleareyed look at the climate-driven
calamities that have beset California, the Caribbean and, most recently,
Texas. It will also require an honest accounting of their great cost,
in both human and financial terms, and of the need to guard against
their recurrence in the years to come.
Nurses applaud introduction of CalCare bill to implement a single-payer system in California
California Nurses Association - February 19, 2021
AB 1400 would guarantee comprehensive, high-quality health care
for all Californians as a human right, leading the nation in the larger
fight for health care justice
Renewing its commitment to the larger fight for health care justice,
the California Nurses Association (CNA) is pleased to sponsor Assembly
Bill 1400 (Kalra), the California Guaranteed Health Care for All Act
(CalCare), which would guarantee comprehensive, high-quality health care
to all California residents as a human right. The establishment of the
CalCare program is an improved Medicare for All-type health care system.
Despite the gains made under the Affordable Care Act, nearly 3
million Californians have no health insurance, while millions more have
insurance that they can’t afford to use because their copays and
deductibles are too high. Meanwhile, for-profit insurance companies are
reporting record-breaking profits, even while the Covid-19 pandemic
continues to ravage California and medical bankruptcies are at an all
time high.
Sponsored by CNA and authored by Assemblymember Ash Kalra, AB 1400
will ensure that all Californians, regardless of employment, income,
immigration status, race, gender, or any other considerations, can get
the health care they need, free at the point of service.
“From our experiences caring for patients, we nurses have known the
need for and fought for decades for everyone to have guaranteed health
care through a system like CalCare,” said Bonnie Castillo, RN and
executive director of California Nurses Association and the national
nursing organization with which it is affiliated, National Nurses
United. “The Covid pandemic has just underscored the desperate societal
need for this program NOW. CalCare will ensure that public health is the
priority of our health care system, not making a buck for insurance
corporations.”
CNA nurses have been at the forefront of the fight to guarantee
health care as a right for all Californians since 1994, when they led
the charge for Prop. 186, a ballot measure that would have implemented a
single-payer system in California. Since then, nurses have continued to
advocate for guaranteed health care for all, knowing all too well the
failings that come with a health care system that places profits ahead
of patients.
“Thank you to Assemblymember Kalra for his leadership in proposing
CalCare, a program that will transform the lives of all people in
California, bringing them security, stability, and health care as the
human right we all agree it is,” said Stephanie Roberson, government
relations director for California Nurses Association.
Most recently, CNA launched the campaign to win CalCare with a day of
action on Feb. 6, working with volunteers throughout California to host
23 car caravans throughout the state, which attracted more than a
thousand participants in total.
The CalCare program would be a truly transformative change to
California’s health care system. In addition to guaranteeing health care
to all Californians, it would save families and businesses thousands in
annual health care costs by cutting out the bloat, waste, and
inefficiencies of our fragmented, for-profit insurance system.
Californians overwhelmingly support the transition to a single-payer
health care system: 57 percent of all Californians supported replacing
private insurance with guaranteed coverage provided by the government --
even before the Covid-19 pandemic caused millions of Californians to
lose their jobs and employer-provided health insurance.
“A single-payer health system represents the belief that health care
is truly a human right. Our current system results in unjust outcomes
and these inequities are underscored especially now, exacerbating
economic downturns for working families who have lost their income and
meaningful access to health care,” said Assemblymember Ash Kalra. “We
will have a long fight ahead in fixing our broken system, but this bill
will set us on a real path towards a single-payer system and affirms the
policy that would save lives, decrease suffering, and improve public
health in California.”
With the introduction of AB 1400, CNA is excited to organize
throughout the state to win CalCare and invites anyone interested in
joining nurses to fight for the bill’s passage to a strategy call for
activists on Thursday, Feb. 25, at 5 p.m. PT. Please sign up to attend
at https://bit.ly/febcalcarecall
A
new study finds that dealing with health insurance administrators costs
the U.S. economy billions in wasted work time and lost productivity.
|byEdmund L. Andrews - Insight by Stanford Business - February 23, 2021
Seems everybody has a horror story about health insurance: Kafkaesque
debates with robotic agents about what is and isn’t covered. Huge bills
from a doctor you didn’t know was “out of network.” Reimbursements that
take months to process.
It’s no secret that health care in the United States is tangled in
wasteful red tape. A study in 2019 estimated that administrative
complexity was the single biggest source of waste in health care — bigger even than fraud or over-pricing — and imposes an annual cost of $265 billion.
The true extent of that waste, according to a new study led by Jeffrey Pfeffer
at the Stanford Graduate School of Business, is even more shocking.
Pfeffer and his colleagues found that administrative “sludge” in health
care insurance costs employers and the economy billions of dollars in
squandered work time, employee stress, absenteeism and reduced
productivity.
Specifically, the researchers estimate, the economy loses $21.6
billion a year simply from the time employees spend on the phone with
health insurance representatives. On top of that, the study estimates
that companies lose $26 billion a year from extra absence on the part of
employees who have to deal with health benefits administrators, and $95
billion from the reduced productivity that arises because people who
spend time on the phone with health insurers are less satisfied with
their jobs. All of those dead-weight losses to the economy could be
diminished if employers held benefits administrators accountable for
reducing administrative hassles in the system.
The Drain on Productivity
If that just sounds like grousing, it’s not. Pfeffer teamed up with
researchers at Gallup, the polling company, to assess how much time
employees spend on the phone with benefit administrators and how those
encounters affect their work.
“Until now, most of the research on health care sludge has focused on
the paperwork costs incurred by health care providers such as doctors
and hospitals,” Pfeffer says. “Our new twist, which I can’t believe no
one looked at before, is how much employee time is wasted and the
measurable effect of that time on employee stress, burnout, increased
absence, and diminished job satisfaction.”
Pfeffer’s coauthors are Dan Witters, research director at Gallup’s
National Health and Well-Being Index; Sangeeta Agrawal, a Gallup
researcher in predictive analytics; and James K. Harter, chief scientist
at Gallup’s workplace management practice.
The team began by polling people on how much time they had spent on
the phone in the prior week with health insurance administrators. The
researchers used data collected from surveys of the Gallup Panel, a
100,000-member group formed in 2004 and designed to represent the entire
U.S. adult population. The surveys employed in this study had a sample
size of about 6,200 people.
There are weeks, of course, when people don’t talk to their health
insurers at all. But on average, the respondents reported spending
almost three minutes of working time and 5.5 minutes in total during the
prior week on such calls. Extrapolating that to some 130 million
full-time workers in the United States, at an average cost per worker of
$37 per hour, those phone calls added up to a nationwide cost of $414
million per week in lost work time. Part-time employees contributed
another $50 million in lost work per week. All told, the annual cost of
lost work amounted to $21 billion — frittered away while talking on the
phone with health insurance representatives.
“It’s simple arithmetic,” Pfeffer says.
The Impact on Worker Morale
The next step was to look at whether those encounters made people more dissatisfied and less engaged in their work.
Sure enough, the people who had talked with a benefits administrator
were significantly less satisfied with their jobs and more likely to be
absent from work.
Even when the researchers controlled for people’s self-reported
health, those who had talked with a benefits person the previous week
were 10% less likely to be satisfied with their workplace and 14% less
likely to feel engaged. They were also more likely to make their
companies pay for their discontent: Employees who had talked with a
benefits administrator were 35% more likely to be absent a day or more
from work, amounting to a nationwide annual cost of $26 billion.
Drawing on extensive research about the link between workers’ job
satisfaction and productivity, Pfeffer and his colleagues estimate that
the reduced job satisfaction coming from spending time on the phone with
health insurers is costing the country an additional $95 billion
annually in reduced productivity.
Pfeffer acknowledges that he plunged into the issue because of his
own frustration with Blue Shield of California, an experience he writes
about in his forthcoming book, I’ve Got the Blues: What a Year with
California Blue Shield Taught Me About What’s Wrong with America’s
Employer-Sponsored Health Care — and How to Fix It.
Who’s Really to Blame?
Pfeffer says the fault lies less with insurance companies than with
the companies that hire them and then fail to hold them accountable.
“CEOs are the ones who should care about this, but they’re only
interested in how to reduce direct medical costs,” he says, “not
realizing that the indirect costs of turnover, absenteeism, and
diminished productivity are many times the direct costs of ill-health.
“We don’t hold these outside administrators accountable. We don’t
measure how long it takes them to process claims, or how much
aggravation they’re causing employees, or whether they are in fact
helping with recruitment and retention through their actions. If you
don’t hold health insurers accountable, you shouldn’t expect them to do a
particularly good job — and they don’t.”
The upshot, Pfeffer continues, is that companies end up paying huge
sums of money for employee health care benefits that don’t provide
increased employee morale because of the burdens imposed by insurers.
“Companies say they offer health insurance to attract and retain
talent, but they’re offering a benefit which is administered so that it
often doesn’t feel like a benefit,” says Pfeffer. “If employers would
select better-performing health insurers and get rid of those that are
administratively inefficient, they would get more value for the money
they are spending.”
I’ve just finished reading a new book that I think will be of great value to anybody interested in better understanding American health care policy, and why it’s so complex, dysfunctional and hard to change. It’s titled “Medicare For All: A Citizen’s Guide”, written by Abdul El-Sayed and Micah Johnson, and published by the Oxford University Press.
It’s scope and accessible style of writing make it a valuable resource for even a lay audience unfamiliar with the wonky policy jargon that often acts as a barrier to a clear understand of health policy in the US. It explores the history, policy and politics of American health care, and is very much up to date, even through the Covid-19 pandemic. It describes the barriers to reform of our broken health care system, and strategies (and the odds for success) for reform.
Highly recommended!
- SPC
How Trump Affected Americans’ Health
by Giovanni Rossonello - Lancet - February 11, 2021
Former President Donald Trump stands accused of inciting a riot that left at least five peopledead and more than 100 police officers injured.
But according to a new report from The Lancet, a respected medical journal, that’s just the tip of the iceberg when it comes to the harm that Trump did to public health during his time in office.
Released today, the 49-page report ticks off the health effects of Trump’s policies on everything from the environment to taxes to Covid-19. And the results aren’t pretty.
Soon after Trump took office in 2017, The Lancet established the Commission on Public Policy and Health in the Trump Era to study the health impact of his decisions in the White House. Over the past four years, the commission analyzed his policies as they took shape while seeking to place them in a broader historical context.
They found that Trump’s mismanagement of the coronavirus pandemic caused tens of thousands of deaths that might have been avoided if the country’s response had been more effectively coordinated.
“I think the huge number of deaths from Covid, compared to the other G7 wealthy nations, was striking,” said Steffie Woolhandler, a co-chairman of the committee and a distinguished professor at Hunter College in New York.
But even before the pandemic, the report found, Trump’s attempts to dismantle the Affordable Care Act had increased the number of uninsured Americans by two million to three million people.
His trillion-dollar tax cuts primarily benefited high-income Americans, while stripping the federal government of resources that it had used to pay for social-welfare programs.
“Even prior to the pandemic,” said Woolhandler, a physician, “the United States’ policies had so thoroughly failed to provide the conditions to protect health that 461,000 people who died in 2018 would have survived if our death rate were the same as other healthy nations.”
Yet she noted that many of the United States’ public health problems predated not only the pandemic, but also the Trump administration. In many cases, the authors wrote, the health decline under Trump was only a continuation of a broader trend — one that seems to have begun in the early 1980s.
“In 1980, life expectancy in the United States was the same as in all our developed nation counterparts — Germany, France, Japan,” said Kevin Grumbach, a member of the commission and a professor at the University of California, San Francisco. “Every year since 1980, the U.S. started falling farther and farther behind these other nations. So now we are three or four years behind the average life expectancy of these other nations.”
Grumbach, who is also a physician, said that over the same period, the cost of health care had risen far more quickly in the United States than in other nations — a trend that Trump contributed to. The report found that his administration increased the privatization of government health programs like Medicare, most likely leading to a rise in costs for consumers.
The report also concluded that by loosening scores of regulations, Trump caused environmental harm that led to the deaths of over 22,000 people in 2019 alone. That was significantly more than had died for similar reasons in 2016.
“That was very surprising, because it’s one area the United States has been improving on in recent decades,” Woolhandler said. “And Trump very quickly managed to reverse the progress.”
This report by the Lancet
Commission on Public Policy and Health in the Trump Era assesses the
repercussions of President Donald Trump's health-related policies and
examines the failures and social schisms that enabled his election.
Trump exploited low and middle-income white people's anger over their
deteriorating life prospects to mobilise racial animus and xenophobia
and enlist their support for policies that benefit high-income people
and corporations and threaten health. His signature legislative
achievement, a trillion-dollar tax cut for corporations and high-income
individuals, opened a budget hole that he used to justify cutting food
subsidies and health care. His appeals to racism, nativism, and
religious bigotry have emboldened white nationalists and vigilantes, and
encouraged police violence and, at the end of his term in office,
insurrection. He chose judges for US courts who are dismissive of
affirmative action and reproductive, labour, civil, and voting rights;
ordered the mass detention of immigrants in hazardous conditions; and
promulgated regulations that reduce access to abortion and contraception
in the USA and globally. Although his effort to repeal the Affordable
Care Act failed, he weakened its coverage and increased the number of
uninsured people by 2·3 million, even before the mass dislocation of the
COVID-19 pandemic, and has accelerated the privatisation of government
health programmes. Trump's hostility to environmental regulations has
already worsened pollution—resulting in more than 22 000 extra deaths in
2019 alone—hastened global warming, and despoiled national monuments
and lands sacred to Native people. Disdain for science and cuts to
global health programmes and public health agencies have impeded the
response to the COVID-19 pandemic, causing tens of thousands of
unnecessary deaths, and imperil advances against HIV and other diseases.
And Trump's bellicose trade, defence, and foreign policies have led to
economic disruption and threaten an upswing in armed conflict.
Although
Trump's actions were singularly damaging, many of them represent an
aggressive acceleration of neoliberal policies that date back 40 years.
These policies reversed New Deal and civil rights-era advances in
economic and racial equality. Subsequently, inequality widened, with
many people in the USA being denied the benefits of economic growth. US
life expectancy, which was similar to other high-income nations' in
1980, trailed the G7 average by 3·4 years in 2018 (equivalent to 461 000
excess US deaths in that year alone). The so-called war on drugs
initiated by President Richard Nixon widened racial inequities and led
to the mass incarceration of Black, Latinx, and Indigenous people.
Overdose deaths soared, spurred by drug firms' profit-driven promotion
of opioids and the spread of despair in long-afflicted communities of
colour and among working-class white people. Market-oriented health
policies shifted medical resources toward high-income people, burdened
the middle class with unaffordable out-of-pocket costs and deployed
public money to stimulate the corporate takeover of vital health
resources.
The Commission applauds President Joe
Biden and Vice President Kamala Harris for rejoining WHO and the Paris
Climate Agreement, and for other steps they have taken to rescind some
of President Trump's health-harming executive actions. But the new
administration and Congress must go beyond simply repairing Trump's
damage. They must initiate thoroughgoing reforms to reverse widening
economic inequality and the neoliberal policy drift that pre-dated
Trump, and redress long-standing racism—root problems that harm health
and have fomented threats to US democracy. Additionally, forceful action
is needed to forestall environmental disaster and strengthen public
health infrastructure.
Reducing
economic inequality will require raising taxes on the wealthy and using
the proceeds to strengthen social, education, nutrition, and health
programmes. Those programmes should avoid segregating the poor, and
instead encompass all people in the USA to bolster the solidarity that
is key to securing broad and continuing popular support. Government
should stop funnelling expenditures through private firms whose
profit-seeking boosts costs and distorts priorities. Hence, a single
payer health-care reform offers the fairest, most effective, and most
efficient route to universal health coverage.
Censure
of Trump's virulent brand of racism is imperative but insufficient. US
leaders must embrace emphatically anti-racist politics and programmes to
dismantle the centuries-old structures that reproduce racial inequity
in health and all other spheres. Ending mass incarceration and reforming
the execrable policing and criminal justice systems that oppress
communities of colour and fill prisons are essential for racial justice.
Additional steps must include vigorous enforcement of voting and civil
rights; large new investments in educational equity, the Indian Health
Service, and minority-serving health and educational institutions; and
compensation for wealth denied to and confiscated from communities of
colour in the past.
Finally, the
president and the Congress must mobilise massive resources to avert
climate catastrophe, address the calamities caused by COVID-19, and
attenuate global inequality. The 3·4% of GDP the USA currently spends on
troops and armaments should be reduced to the 1·4% average of other G-7
nations, with the savings redeployed to address urgent health, social,
and environmental problems at home; reinvigorate the scientific efforts
that are vital to global progress; and fund the four-times increase in
foreign aid needed to reach the level recommended by the UN.
Key messages
During his time in office President Trump:
•
Politicised and repudiated science, leaving the USA unprepared and exposed to the COVID-19 pandemic
•
Eviscerated environmental regulation, hastening global warming
•
Incited racial, nativist, and religious hatred, provoking vigilante and police violence
•
Denied refuge to migrants fleeing violence and oppression, and abused immigrant detainees
•
Undermined health coverage
•
Weakened food assistance programmes
•
Curtailed reproductive rights
•
Undermined global cooperation for health, and triggered trade wars
•
Shifted resources from social programmes to military spending and tax windfalls for corporations and the wealthy
•
Subverted democracy both nationally and internationally
Although
the Trump administration policies posed a uniquely urgent threat to
health, damaging neoliberal policies predated and abetted his
ascendance:
•
Life expectancy in the USA has lagged behind other wealthy nations since 1980 and began falling in 2014
•
The
chronically high mortality of Native Americans started rising in 1999,
while yawning disparities between Black and white people persisted and
progress on racial equity in other domains (eg, education, housing,
income and policing) halted or reversed
•
Substance abuse deaths greatly increased
•
Income and wealth inequality widened
•
Incarceration
increased four-fold, initiated by President Nixon's racially motivated
war on drugs and compounded by harsh laws enacted under Presidents
Reagan and Clinton
•
Welfare eligibility restrictions implemented by President Clinton removed benefits from millions
•
Deindustrialisation
spurred by trade agreements that favoured corporate interests over
labour protections reduced economic opportunity in many regions of the
USA, damaging health and increasing receptivity to racist and xenophobic
appeals
•
Market-based
reforms commercialised and bureaucratised medical care, raised costs,
and shifted care toward high-income US residents
•
Despite
the Affordable Care Act, nearly 30 million people in the USA remained
uninsured and many more were covered but still unable to afford care
•
Funding cuts reduced the front-line public health workforce by 20%
The
Biden administration must cancel Trump's actions and also address the
health-damaging structural problems that were present before Trump's
presidency:
•
Raise
taxes on high-income people and use the proceeds to bolster social,
educational, and health programmes, and address urgent environmental
problems
•
Mobilise against the structural racism and police violence that shorten the lives of people of colour
•
Replace
means-tested programmes such as Medicaid that segregate low-income
people, with unified programmes such as national health insurance that
serve all US residents, aligning the interests of the middle class and
the poor in maintaining excellence
•
Reclaim
the US Government's role in delivering health and social services, and
stop channelling public funds through private firms whose profit-seeking
skews priorities
•
Redirect
public investments from militarism, corporate subsidies, and distorted
medical priorities to domestic and global fairness, environmental
protection, and neglected public health and social interventions
•
Reinvigorate
US democracy by reforming campaign financing, reinforcing voting,
immigration, and labour rights, and restoring oversight of presidential
prerogatives
COVID-19's
facile breach of national boundaries is a reminder of the vulnerability
of even the most powerful nations in an interconnected world, and the
folly of contempt for science, facts, and equity. In years past, the USA
deployed its economic power and scientific prowess in important,
although imperfect, efforts to advance global health. It must rejoin the
global community in a spirit of collaboration, rejecting the notion
that others must fail in order for the USA to succeed.
Congressional Budget Office Scores Medicare-For-All: Universal Coverage For Less Spending
by Adam Gaffney, David Himmelstein and Steffie Woolhandler - Health Affairs Blog - February 16, 2021
For the first time in a quarter century, the Congressional Budget Office (CBO) has undertaken an economic analysis
of single-payer health care reform, also known as Medicare for All. The
more than 200-page working paper, released last month, includes a rich
explanation of methodology together with cost projections for 2030 and
will no doubt serve as an important reference for years to come.
The report makes many sound assumptions but also some questionable
ones that are overly pessimistic. Yet, overall, its bottom-line
estimates should reassure those concerned about the economic feasibility
of single payer: The CBO projects that such reform would achieve
universal coverage, bolster provider revenues for clinical services, and
eliminate almost all copayments and deductibles—even as overall health
care spending fell.
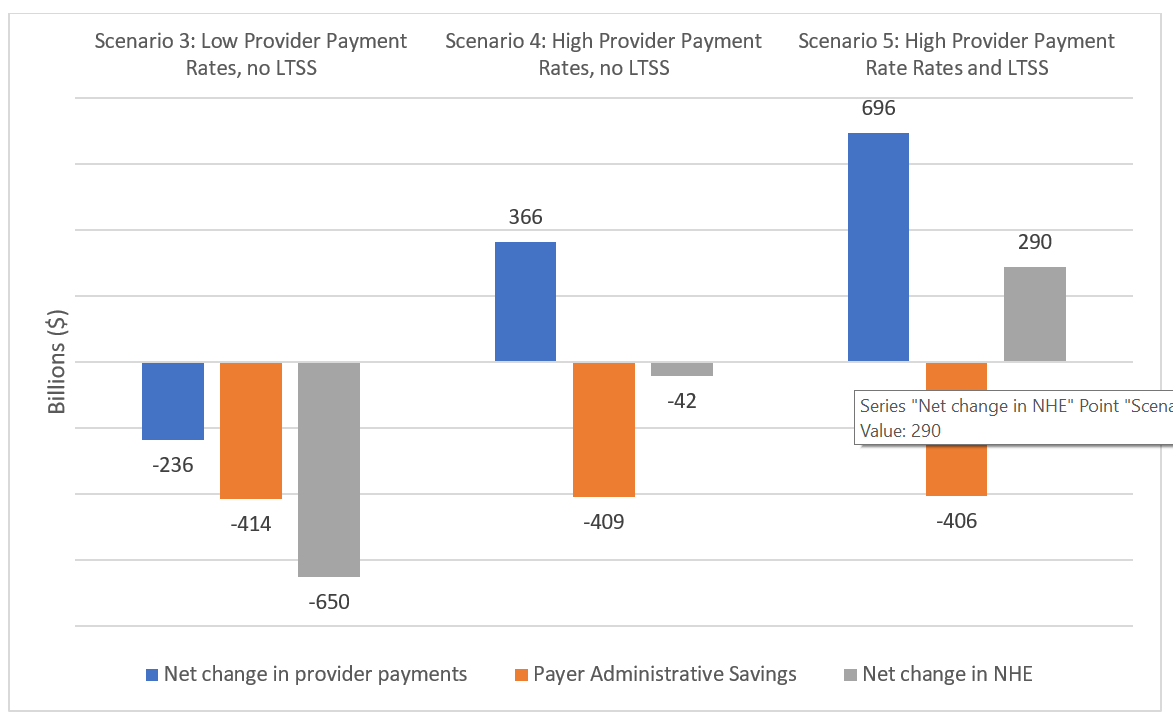
The CBO models costs under five different variants of single payer.
The first four envision universal coverage of all services other than
long-term care, while the fifth incorporates a large expansion of
long-term services and supports (LTSS) for people with disabilities of
all ages. The scenarios vary by patient cost sharing and provider
payment level. Low cost-sharing has no copays or deductibles for medical
services and minimal cost sharing for prescription drugs; under high
cost-sharing, patients with incomes above 150 percent of poverty would
bear about 7.5 percent of costs out of pocket. Low payment rates to
providers would set rates slightly higher than Medicare’s; high rates
would be equivalent to the current average of the rates paid by private
insurers and government programs. The five variants (or scenarios) are
summarized in exhibit 1.
Exhibit 1: Congressional Budget Office’s five single-payer scenarios
We discuss below the CBO’s estimates of single payer’s overall
effects on national health spending, the implications of the estimates
for providers, and the concerns the analysts raise about worsened
“provider congestion” under a single-payer health care system.
Throughout, we point out instances where the CBO’s assumptions differ
from previous, widely publicized analyses, or from provisions included
in the Medicare for All legislation currently in Congress.
CBO’s Estimates Of Single Payer’s Effects On National Health Expenditures
The CBO projects that variants 1–4 of single-payer reform would
reduce national health expenditures (NHE) despite substantial increases
in the use of care triggered by expanded and upgraded coverage. If a
vast new program covering LTSS for all US residents were included
(scenario 5), the CBO estimates that NHE would rise by 4.4 percent above
currently projected spending levels. Exhibit 2 summarizes the CBO’s
spending estimates for the three low cost-sharing scenarios, which are
similar to the Medicare for All bills in Congress.
Exhibit 2: Congressional Budget Office estimates of effect of single
payer on health spending in 2030: low cost-sharing scenarios
How can the use of care rise even as spending falls? Mostly,
according to the CBO, through greater administrative simplicity. As the
CBO notes, traditional Medicare’s administrative overhead accounts for
approximately 2 percent of its total revenue, compared to the 12 percent
overhead of private insurers. Under single payer, the CBO projects,
administrative spending would fall accordingly; overall overhead for the
Medicare for All system is estimated by the CBO at below 2 percent. As
shown in exhibit 2, this translates into around $400 billion annually
(more than $1,000 per capita) in savings under all of the single-payer
variants.
Of note, these evidence-based projections clash with the analyses by the Urban Institute and the RAND Corporation,
which perplexingly assumed much higher administrative overhead under a
single-payer system than under the current traditional Medicare program
or under universal systems abroad.
Implications For Provider Overhead And Revenue
The CBO appropriately projects substantial administrative savings for providers, again unlike many previous analyses. US hospitals and physicians
waste money and time contending with multiple payers, each with its own
complex and varying coverage rules and payment procedures, formularies,
and so forth. The CBO projects that the share of revenues that
hospitals spend on administration would fall from 19 percent at present
to 12 percent under single payer; that physicians’ administrative
overhead would fall from 15 percent to 9 percent; and that the
administrative expenses of other medical providers (for example,
dentists, home health agencies, and hospices) would fall from 9 percent
to 6 percent. In addition, it estimates that physicians and nurses would
spend less time on administrative activities, freeing up 4.8 percent of
physicians’ work hours and 18.4 percent of nurses’ work time. These
assumptions build on a large evidence base showing high administrative overhead among US health care providers relative to other nations.
The CBO assumes that single payer would allow providers to keep these
savings on administration and billing, and use the resources freed up
to provide more care. Hence, providers’ administrative savings do not
appear as savings in exhibit 2. In effect, the CBO interprets these
efficiencies as reductions in providers’ costs that would enable them to
deliver a greater quantity of services for a given amount of revenue.
Consequently, the “net change in provider payments” shown in exhibit 2
doesn’t fully account for the extra resources made available to
hospitals, doctors, and other providers under Medicare for All. In
contrast, exhibits 3 and 4 present our estimates of single payer’s
financial impacts on physicians and hospitals, incorporating CBO
projections of providers’ savings on administrative spending and
physicians’ and nurses’ time.
As exhibit 3 demonstrates, payments to clinicians would rise in all
five scenarios according to CBO estimates. We estimate this translates
into an additional $39,816–$157,412 in revenue per practicing physician.
At the same time, physicians’ practice overhead would shrink under
single payer, increasing practices’ take-home income. Such a windfall,
in our view, may be excessive, at least for some providers. (Disclosure:
The authors are all physicians).
Source: Authors’ analysis of the Congressional Budget Office’s (CBO’s) Single-Payer Health Care Systems Team. How
CBO analyzes the costs of proposals for single-payer health care
systems that are based on Medicare’s fee-for-service program.
Washington (DC): CBO; 2020 Dec. Note: *Based on Association of American
Medical Costs estimate of 840,000 practicing physicians in 2030 and the
assumption that physician payments account for 77.78 percent of payments
in the “Physician and other Clinical Service” category, as they did in
2018 according to the National Health Expenditure Accounts.
For hospitals, the CBO estimates that gross revenue would fall by
$187 billion under the “low pay” scenario but rise by $144 billion under
the high-payment scenario. Again, these figures do not give the full
picture of the impact on hospitals’ bottom lines, given the CBO’s
projections that single-payer reform would shrink hospitals’ spending on
administration and would also free up substantial amounts of nursing
time that is currently devoted to payment-related tasks. The CBO’s
estimates suggest that hospitals would save $143 billion to $166 billion
on administration and an additional $59 billion on freed-up nursing
time, resources that could be redirected to clinical care (exhibit 4).
Overall, building on the CBO’s projections, we estimate that hospitals’
clinical funding would change little (rising by $15 billion) under the
low-payment scenario or increase substantially, by $369 billion, under
the higher-payment one.
Exhibit 4: Modeling Congressional Budget Office’s low cost-sharing
scenario: ramifications for hospitals’ revenues and clinical operating
budgets
Source: Authors’ analysis of the Congressional Budget Office’s (CBO’s) Single-Payer Health Care Systems Team. How
CBO analyzes the costs of proposals for single-payer health care
systems that are based on Medicare’s fee-for-service program.
Washington (DC): CBO: 2020 Dec. Notes: **Based on the CBO estimate that
hospitals’ spending on administration (excluding registered nurse
(RN)and licensed practical nurse (LPN) time spent on administration)
would be reduced from 19 percent to 12 percent of hospital revenues.
***Based on (1) Bureau of Labor Statistics estimate of number of RNs and
LPNs employed in hospitals and average RN and LPN wages in 2019; (2)
the assumption that benefit costs equal 20 percent of wages; (3) the
assumption that nursing costs would rise at the same rate as overall
hospital costs; and (4) CBO’s estimate that RNs and LPNs devote 23
percent of time to administration and that single payer would reduce
that time by 80 percent.
The large increase in hospital funding that the CBO projects under
the high-payment scenario would, in our view, give an appropriate boost
to many struggling rural and safety-net hospitals but would be excessive
for hospitals that are currently realizing large annual profits.
Additionally, the fee-for-service hospital financing modeled by the
CBO differs from what is envisioned in the Medicare for All bill in the
House of Representatives. The House bill proposes paying hospitals,
nursing homes, and other institutional providers using “global budgets,”
that is, lump sums to cover all of their operating activities. This is
the model used by Canada and the US Veterans Health Administration.
Global budgeting could allow even greater reductions
in administrative spending by eliminating the need for per-patient
billing altogether. It would also allow payments to match current
operating budgets and facilitate the gradual redistribution of funding
among hospitals, directing more resources to communities most in need.
The global budgeting approach, however, would require separate
financing of capital expenditures (as in Canada and some European
nations), which again is an approach explicitly included in Medicare for
All bills in Congress but not in the CBO report. Such regulated capital
financing, in turn, could help regulate cost growth in the longer term
by avoiding investments in duplicative but profitable high-tech
facilities that encourage the delivery of low- or no-value care.
Hence, the CBO’s decision to model a system that used fee-for-service
payments for hospitals and other institutional providers rather than
global budgets with separate capital financing leads it to underestimate
single-payer savings in the short term and to ignore potential
longer-term savings and improvements in the distribution of hospital
infrastructure. That caveat aside, an important takeaway from the CBO’s
analysis is that, overall, providers would see stable or even increased
funding for patient care under single payer, even while overall health
spending fell.
Provider Congestion?
While the CBO report foresees greatly improved financial access to
care under single payer, it raises the specter of “provider congestion,”
that is, greater difficulty making appointments or rising waiting times
under single payer. Because such reform would newly cover the uninsured
and improve coverage for most other people, the CBO projects large
increases in the demand for care, and hence use. However, it projects
that not all of the demand could be met because of supply constraints,
for example, the finite number of doctors, nurses, and hospital beds.
Consequently, the report predicts increased “provider congestion” that
would cause some foregone care.
This prediction, however, is out of touch with clinical reality, an issue we recently explored in Health Affairs.
The CBO’s approach to supply constraints is only half right. There is
little question that, as the CBO assumes, a finite supply of health care
providers constrain utilization increases after coverage expansions: As
we have demonstrated,
in nation after nation, universal coverage expansions have led to
modest, or even no, societywide increases in use. Increased use by the
newly covered has usually been partially or fully offset by small
reductions in use among the well-covered or well-off.
Yet, these small reductions appear to be mostly due to the reduced provision of low-value care. Two econometricstudies
found that offsets after coverage expansion reflect reductions in the
amount of wasteful care provided to the already insured. Similarly, studies
by the Dartmouth Group indicate that the volume of elective and
low-value care increases when the supply of doctors and hospital beds
rise—a phenomenon called supplier-induced demand. In other words, faced
with an increase in demand for care, providers prioritize their time and
services, delivering more high-value care while reducing the provision
of low- or no-value services.
Characterizing such offsets as “unmet demand” or “congestion” is
hence misleading. It mirrors previous forecasts of “patient pileups”
when Medicare was first implemented—forecasts that proved incorrect. In
the US today, nearly one-third
of all health care delivered is unnecessary or wasteful. Overprovision
is common. If coverage expansion leads to some attenuation in
supplier-induced demand, all the better.
A Notable Omission
Finally, while the CBO projects reductions in health spending in four
out of five single-payer scenarios, as noted, it projects substantial
increases in federal spending that would replace all private insurance
premiums and nearly all out-of-pocket health care costs. Yet, there are
also substantial savings for state and local governments with
single-payer reform. The CBO’s brief mention of the savings likely to
accrue to these governments (and their taxpayers) omits probable savings
from no longer having to bear the costs of public employees’ health
insurance (projected to total $318 billion in 2030), as well as about
$162 billion in savings on other health programs. These, together with
savings on Medicaid (which the CBO does remark on), would bring state
and local governments’ total savings from single payer to about $800
billion in 2030 alone, reductions that provide important context for the
CBO’s estimates of increased federal government expenditures.
The Economics Of Single-Payer Financing: CBO’s Bottom Line
Overall, the CBO report provides one of the most detailed
explorations to date of the economics of single-payer financing. As we
have noted, it makes many sound assumptions, particularly about payer-
and provider-side administrative savings. At the same time, it adopts
some unfavorable assumptions about the structure of single-payer reform
(including some that conflict with key provisions of the Medicare for
All bills in Congress), projects excessive windfalls for some providers,
and asserts clinically nescient portrayals of “unmet demand.”
Nonetheless, the bottom line of the CBO analysis—that universal coverage
can be affordably achieved even as benefits are expanded and cost
sharing all but eliminated—should reinvigorate debate over such reform.
by Austin Frakt and Tynan Friend - The Incidental Economist - February 10, 2021
The complexity
of Medicare Advantage (MA) physician networks has been well-documented,
but the payment regulations that underlie these plans remain opaque,
even to experts. If an MA plan enrollee sees an out-of-network doctor,
how much should she expect to pay?
The answer, like much of the
American healthcare system, is complicated. We’ve consulted experts and
scoured nearly inscrutable government documents to try to find it. In
this post we try to explain what we’ve learned in a much more accessible
way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third
of the 60+ million Americans covered by Medicare are enrolled in MA
plans. These plans, subsidized by the government, are governed by
Medicare rules, but, within certain limits, are able to set their own
premiums, deductibles, and service payment schedules each year.
Critically,
they also determine their own network extent, choosing which physicians
are in- or out-of-network. Apart from cost sharing or deductibles, the
cost of care from providers that are in-network is covered by the plan.
However, if an enrollee seeks care from a provider who is outside of
their plan’s network, what the cost is and who bears it is much more
complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers,
which constitute about 97% of all physicians in the U.S., accept
Medicare Fee-For-Service (FFS) rates for full payment of their services.
These are the rates paid by TM. These doctors are subject to the fee
schedules and regulations established by Medicare and MA plans.
Non-participating providers
(about 2% of practicing physicians) can accept FFS Medicare rates for
full payment if they wish (a.k.a., “take assignment”), but they
generally don’t do so. When they don’t take assignment on a particular
case, these providers are not limited to charging FFS rates.
Opt-out providers
don’t accept Medicare FFS payment under any circumstances. These
providers, constituting only 1% of practicing physicians, can set their
own charges for services and require payment directly from the patient.
(Many psychiatrists fall into this category: they make up 42% of all
opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So,
if an MA beneficiary goes to see an out-of-network doctor, by whom does
the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member
willingly seeks care from an out-of-network provider, the member
assumes full liability for payment. That is, neither the HMO plan nor TM
will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies,
and must be disclosed to the patient before any services are
administered. If the provider is participating with Medicare (in the
sense defined above), they charge the patient no more than the standard
Medicare FFS rate for their services. Non-participating providers that
do not take assignment on the claim are limited to charging the
beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states
further restrict this. In New York State, for instance, the maximum is
105% of Medicare FFS payment.) In these cases, the provider charges the
patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare,
there are no limits to what they can charge for their services. The
provider and patient enter into a private contract; the patient agrees
to pay the full amount, out of pocket, for all services.
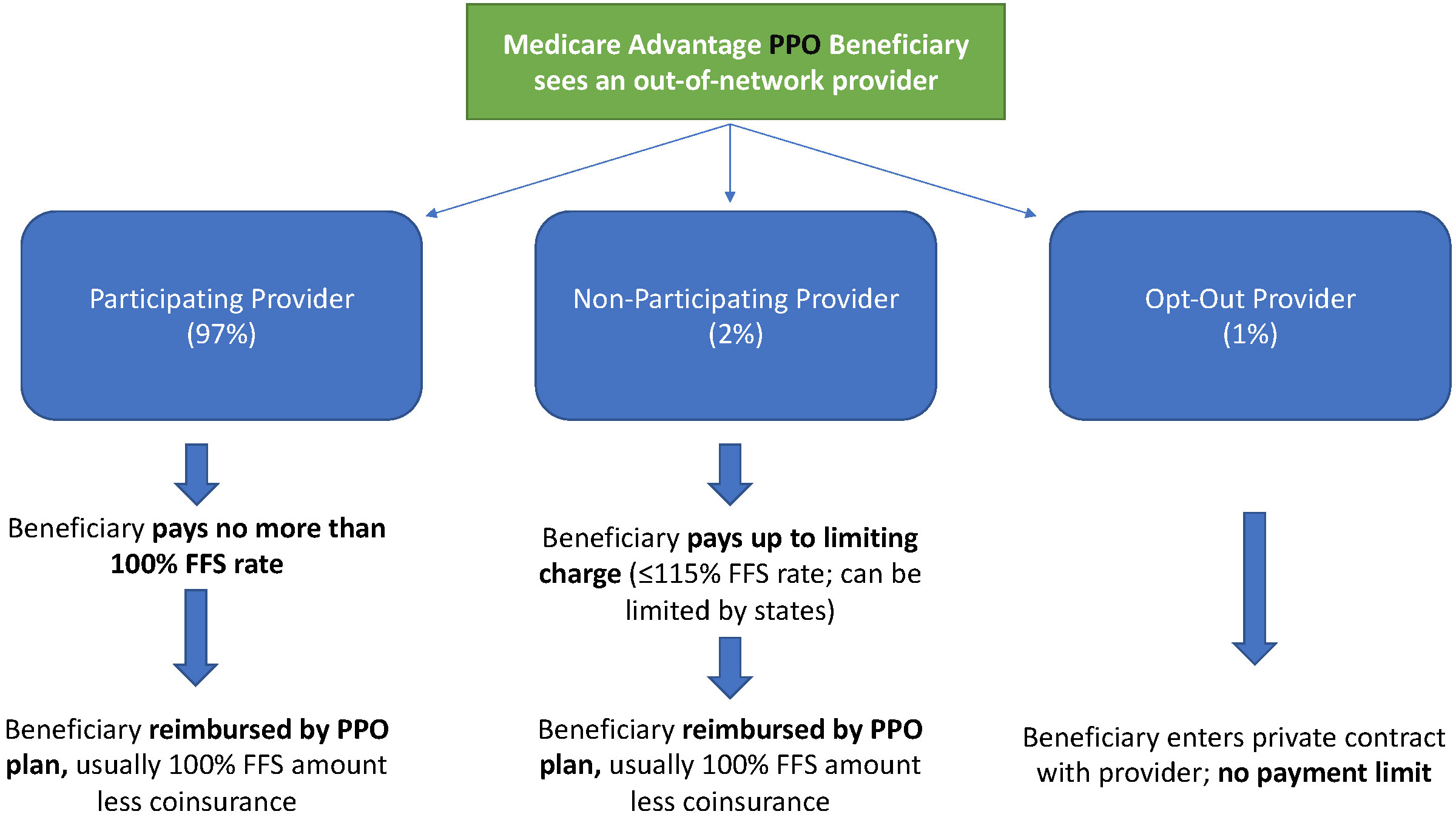
Figure 1: MA HMO Out-of-Network Payments
MA PPO plans operate slightly differently. By nature of the PPO plan,
there are built-in benefits covering visits to out-of-network
physicians (usually at the expense of higher annual deductibles and
co-insurance compared to HMO plans). Like with HMO enrollees, an
out-of-network Medicare-participating physician will charge the PPO
enrollee no more than the standard FFS rate for their services. The PPO
plan will then reimburse the enrollee 100% of this rate, less
coinsurance. (See Figure 2.)
In contrast, a
non-participating physician that does not take assignment is limited to
charging a PPO enrollee 115% of the Medicare FFS amount, which can be
further limited by state regulations. In this case, the PPO enrollee is
also reimbursed by their plan up to 100% (less coinsurance) of the FFS
amount for their visit. Again, opt-out physicians are exempt from these
regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare)
and the provider happens to be out-of-network for the MA plan
(regardless of HMO/PPO status), the plan must cover the services at
their established in-network emergency services rates.
The second
caveat is in regard to the declared public health emergency due to
COVID-19 (set to expire in April 2021, but likely to be extended). MA
plans are currently required
to cover all out-of-network services from providers that contract with
Medicare (i.e., all but opt-out providers) and charge beneficiaries no
more than the plan-established in-network rates for these services. This
is being mandated by CMS to compensate for practice closures and other
difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside
of the pandemic and emergency situations, knowing how much you’ll need
to pay for out-of-network services as a MA enrollee depends on a
multitude of factors. Though the vast majority of American physicians
contract with Medicare, the intersection of insurer-engineered physician
networks and the complex MA payment system could lead to significant
unexpected costs to the patient.
'I don't make enough': the financial cost of having Covid in the US
by Amanda Golpuch - The Guardian - February 12, 2021
Covid-19 allowed for an experiment in US healthcare: what if doctor’s visits and hospitalizations didn’t cost people money?
In
response to the pandemic, major health insurers volunteered to cover
coronavirus testing and treatment for their paying customers and the
government introduced programs to make care more affordable. But a year
after coronavirus was first identified in the US, those assurances
haven’t played out as planned.
A program to help the country’s 28.9 million uninsured has been riddled with problems,
such as patients not knowing which healthcare providers are actually
participating in the scheme. Undocumented immigrants have largely been
excluded from aid. The complexities of long Covid, when people
experience symptoms for months, have challenged patients and providers.
And health insurers still control what gets covered and for how long.
To better understand these disparities, the Guardian spoke to six people about the financial cost of Covid-19.
Mellisa Arredondo Moncibaiz, 51, Texas: $633.32
Out-of-pocket costs: $572.32;. Premium: $61 (for one month)
Mellisa
Arredondo Moncibaiz’s financial stress is tangled up with grief. Six of
her friends and relatives have died from Covid-19 – four of them in
January. “It’s just horrible all around,” she said.
The Wichita
Falls, Texas, resident had Covid at the end of October and spent five
days in the hospital, resulting in a $42,096 bill. The hospital billed
for more than 200 different items – from an $11 zinc capsule to $1,080
for each day of heart monitoring.
She is grateful her health
insurance will pay most of the $42,096 bill, but she still has many
sleepless nights thinking about her debts. The $572.32 she owes for her
coronavirus treatment is on top of the $3,689.81 she owes the hospital
because she broke her tailbone in June.
“After insurance, it’s
still $4,200, I don’t make enough to pay that,” said Moncibaiz, who
works in housing. “I just pay what I can, $20 there, $10 there. But now,
I haven’t been able to pay that because I am worried about rent,
utilities.”
To have health insurance, Moncibaiz pays a $61 premium each month – only a few insurers included premium relief in their Covid assistance.
Her deductible, what people must pay before the insurance kicks in, is
$2,550. After hitting that, insurance covers 80% of her medical costs.
Moncibaiz
said the debt is causing anxiety and depression, which she hasn’t
sought treatment for because of its price tag. She called the $600
stimulus checks the government sent in January “a kick in the teeth”.
The things which have helped the most, she said, are her understanding
landlord and the national pause on federal student loan payments.
“I am just working to keep my head above water,” she said.
Baldhead Phillips, 51, Georgia: $100,000
Uninsured
Atlanta-based
comedian Baldhead Phillips was hospitalized with Covid-19 for two weeks
in March, and each day watched as other patients were wheeled away on
gurneys after succumbing to the illness.
Doctors sent him home
with an order to use $200-a-month oxygen therapy, prescriptions for 11
drugs and new diagnoses of high blood pressure and heart failure.
“I
got home, got the exhaustion, got into bed and the first and last
thought in my mind was I just spent a lot of money to buy this stuff,
and this is not a cure, it’s just to let me live a little longer and see
how it’s going to go,” Phillips, 51, said.
Two days later,
Phillips received a $15,000 bill from the hospital. More bills followed
and Phillips said they have so far totaled more than $100,000.
Phillips doesn’t have insurance and is on the hook for the entire bill.
He has been able to cover some of the costs with help from a GoFundMe online fundraiser and other contributions from fans and friends, but his income is a fraction of what it used to be.
He
hasn’t been able to work as a standup because of coronavirus
restrictions and has stopped his second job as an Uber driver. “I’m so
stressed out about that but at the same time my family is saying, don’t
worry about bills, worry about getting better,” Phillips said.
Last
spring, Phillips was skeptical about the seriousness of Covid. Now, he
uses his public platform to warn about how grave it can be. Phillips
said: “I crack jokes for a living, but this is no joke at all.”
The
government’s nationalized health insurance program for seniors,
Medicare, has kept money at the back of Ellen’s mind while she struggles
with long Covid.
She pays $150 for the coverage each month and has spent less than $100
since she contracted Covid in April on prescription drugs.
But
Ellen, who asked not to use her last name for privacy, has had Covid
symptoms for 10 months – including 128 days of nonstop headaches.
“I
still have fatigue, right now I am laying down in bed, a shower will
wipe me out,” she said from her home in Littleton, Colorado. “I still
have brain fog, after we have this talk, I will be exhausted.”
The
66-year-old has seen a battery of specialists to address the lingering
symptoms, and with Medicare, a government health plan for people 65 and
older, the appointments are covered.
Like most Medicare
beneficiaries, Ellen has supplemental coverage which reduces costs of
things like prescription drugs – she estimates she has spent under $100
on those since April. “It’s fantastic,” she said.
Costs are higher
for the 6 million Medicare beneficiaries who don’t have supplementary
coverage to cover prescriptions, co-pays for doctors’ visits and other
medical care.
Adina
Gerver’s March Covid infection has left her with lingering symptoms
including debilitating fatigue, a nerve system condition and a blood
clot in her right lung.
“I am earning very little right now,
because I am working very little, because I am tired all the time,” said
Gerver, who said she’s relying on financial help from family.
The
41-year-old is being treated by specialists at the Mount Sinai Post
Covid Care Center in New York City. She owes $279.87 of the center’s
$3,900 bill for some of the treatments and tests she had in the autumn
and she has yet to receive bills for all the care she’s received.
Gerver
has Cobra, a government program which allows people to continue with
the insurance they had at their previous employer. Since August, she has
paid $1,000 a month in premiums. Before that, her premiums were about
$800. Separately, once she hits her $3,250 deductible, her plan pays for
100% of her medical expenses.
Then there were the other costs,
such as $20 for a pulse oximeter and spending more on ride-shares to get
around the city. Friends and family also bought her a shower chair, bed
desk and support pillow, which together are at least $100.
Gerver
suspects a government marketplace health insurance plan would cost less
than Cobra, but she doesn’t know if the care she needs for long Covid
would be covered.
The process of navigating health coverage in the
US can be frustrating and time-consuming at the best of times – when
coupled with severe fatigue, it was too much. “I could not get it
together to call them,” Gerver said.
She was also too tired to
fight a recent mystery bill - a month’s supply of the blood thinner she
paid $35 for on 31 December, cost her $491.98 in January.
Yaquelin Valencia, 29, California: $2,000
Out-of-pocket costs: $2,000. Premium: $0 (for one month)
When
Yaquelin Valencia had Covid in July, her biggest worry was how to
continue supporting her undocumented family members, especially as the
main provider for her parents.
“I was concerned a little about my
health, but I was more worried about my parents because I am their sole
provider,” said Valencia, who lives in California’s Bay Area.
The
29-year-old is a recipient of Daca, the temporary protection from
deportation for people who were brought to the US as children without
legal papers. Daca allowed her to collect unemployment when she was laid
off in April and get health insurance when she got a new job in June as
a community organizer in La Red, an immigrant rights campaign by the
advocacy group Faith in Action.
“I felt this sense of security that I know others don’t have because of status,” said Valencia.
In
the past, if Valencia needed to see a doctor, she would have to go to
the hospital because she didn’t have insurance. She still owes hospitals
thousands of dollars from the 18 years she didn’t have health
insurance.
Luckily, her Covid infection was mild. She saw a doctor
online and treated her sore throat, fever, fatigue and loss of appetite
with vitamins, sleep medication and other home remedies. She also spent
extra money to stay in an Airbnb while her apartment was sanitized and
to get food delivered for her and her parents, who she lives with,and
are at high risk for severe Covid.
She estimates that extra spending and medicine set her back $2,000.
Catalina Morales, 29, Minnesota: $5,000
Out-of-pocket costs: $5,000
Catalina Morales has spent about $5,000 on Covid care, even though she never had it.
Late
last year, she and her sister traveled from Minnesota to Chicago to
care for five close family members who had severe Covid-19 infections.
This includes her mom and another sister, who were hospitalized for more
than a week.
Meanwhile, Morales’s brother-in-law battled Covid at
home and took care of the couple’s two children, without paid sick
leave because he is undocumented. To help cover the family’s rent and
food, plus the sisters’ travel, Morales fundraised $5,000 by contacting
people she knows.
Morales, a Daca recipient and manager for the La
Red immigrant rights campaign, said the fundraising was only possible
because she is an activist and is familiar with the networks she could
tap to get help.
“Your regular undocumented immigrant doesn’t know
or doesn’t have those relationships,” Morales said. “If I didn’t have
that knowledge, my sister would not have paid her rent the last two
months and my sister and I would have had to use credit cards to pay for
all this.”
Those initial costs aren’t the family’s only financial concern.
Morales’s
mother had been living in the US undocumented until she received a visa
for victims of crime, but the paperwork is being processed. The
hospital, therefore, doesn’t consider her a US resident, blocking her
from qualifying for programs to help the uninsured.
The family will owe the hospital the fullbill,
and plans to negotiate to pay in installments. The average charge for
an uninsured Covid-19 patient’s hospitalization is $73,300, according to
the not-for-profit insurance database Fair Health.
Biden moving to withdraw Trump-approved Medicaid work rules
Democrats long complained the rules were illegal and aimed at shrinking health coverage for poor adults.
by Adam Cancryn - Politico - February 11, 2021
Former President Donald Trump listens as former Administrator of the
Centers for Medicare and Medicaid Services Seema Verma speaks during a
news conference Friday, Nov. 20, 2020. | Susan Walsh/AP
The Biden administration on Friday will notify states it plans to
revoke Medicaid work requirements, starting the process of dismantling
one of the Trump administration's signature health policies.
The move is one of several steps that Biden’s health department is
expected to take this week to unravel the contentious work rules long
criticized by Democrats, according to internal documents obtained by
POLITICO.
The documents — which were labeled “close hold” — do not make clear
how quickly Biden will cut off work rules the previous administration
approved in a number of states, which for the first time were allowed to
mandate that some people work or volunteer as a condition of enrollment
in the low-income health care program.
Healthofficials
are also preparing to withdraw the Trump administration’s 2018 letter
that first announced the work requirements policy, and rescind a
separate letter from earlier this year aimed at making it more difficult
for the incoming Biden administration to quickly overturn the policy.
“CMS
has serious concerns that now is not the appropriate time to test
policies that risk a substantial loss of health care coverage or
benefits in the near term,” according to a health department draft
rollout plan entitled “Medicaid Work Requirement Rescission.”
President Joe Biden, who has targeted other Trump health policies as he looks to build on Obamacare,
has long signaled plans to unravel the Medicaid work requirements.
Democrats have criticized the rules as unlawful and aimed at kicking
people off the program’s rolls.
Trump
Medicaid chief Seema Verma, who was critical of Obamacare's expansion
of Medicaid to poor adults and crafted the requirements, argued they
would encourage healthy people to work and help keep state Medicaid
programs financially sustainable.
Biden last
month issued an executive order directing his health department to
identify policies that fail to “protect and strengthen Medicaid.” But
the draft rollout plan obtained by POLITICO points to the coronavirus
pandemic as the central reason for rolling back the work rules, arguing
that the crisis has “greatly increased the risk” that the policy will
lead to “unintended coverage loss.”
“In
addition, the uncertainty regarding the lingering health consequences
of COVID infections further exacerbates the harms of coverage loss or
lack of access to coverage for the Medicaid beneficiaries,” the plan
said.
The move also comes as the
Supreme Court is slated to consider the validity of the work rules on
March 29. Lower courts have so far blocked attempts to institute the
work rules, which led most states with the requirements to halt their
enforcement. Biden's plan to withdraw the work rules could render the
Supreme Court case moot.
Centers for Medicare and Medicaid Services did not respond to multiple requests for comment.
Ten
GOP-led states that applied for the Trump administration's permission
for work rules were approved or “considered approved,” according to the
draft rollout plan. Several more states had sought permission for work
rules but had not been approved before Trump left office.
The
work rules were approved through Medicaid waivers, which allow states
to test ideas for health coverage. A new administration typically can
unwind waivers that it believes does not support Medicaid goals, though
states may protest the decision.
In the final weeks of the Trump administration, Verma asked states to
sign contracts that would establish a lengthy process for unwinding
work requirements and other conservative changes to their Medicaid
programs. Medicaid experts have questioned whether those contracts are
legally enforceable.
The health department onFriday is also planning to scrub some
references to the work requirements program and related documents from
the government's Medicaid website.
Instead, it will post a link to an HHS document entitled “Medicaid
Demonstrations and Impacts on Health Coverage: A Review of the
Evidence.” The document, among other topics, will address the “impact of
work requirements on Medicaid’s commitment to Americans in need,” the
draft rollout plan said.
Only one state, Arkansas, ever fully implemented the Medicaid work
rules. About 18,000 people lost Medicaid coverage in 2018 during the few
months the requirements were in effect, before a judge blocked them.
William Clark and Larry Kaplan: Every Maine resident deserves health care.
Universal healthcare — everyone in, no one out — creates unity and solidarity: foundational aspects of American democracy.
Does anyone in your family lack health insurance? Are you foregoing needed medical care? Have you received a “surprise” medical bill. How do Maine residents answer these questions? In autumn 2019, more than 80 volunteers with Maine AllCare interviewed a sample of 3,864 people from every Maine county and 287 towns. The survey, funded by Maine Health Access Foundation, found that while most respondents had health insurance, 78% labeled their health care coverage is “unaffordable.” Forty-two percent reported that they had delayed treatment because of cost while over half received unexpected medical bills that impacted their finances. Most importantly, 81% said they would support “a publicly-funded healthcare system that covered everyone in Maine.”
Also, medical providers complain that they are handcuffed and overburdened by the healthcare system’s complexity and endless administrative paperwork that does not facilitate care. Rural hospitals are threatened with closure. Today’s pandemic underscores the fact that our current system of health care serves both providers and patients poorly, while exorbitant profits flow to insurance corporations, device manufactures and pharmaceutical companies.
Universal healthcare is both equitable and economically viable. Other wealthy countries cover everyone for half to two-thirds of United States costs. Meanwhile, data show that many countries enjoy health outcomes superior to the United States. Advocacy coalitions and legislatures in other states — notably California, Washington, Minnesota and New York — are exploring implementation of universal healthcare. If implemented, these proposals provide more comprehensive benefits than the present ACA plans.
Locally, the Maine Center for Economic Policy examined in 2019 how a hypothetical universal healthcare system would work in Maine. The MECEP study analyst and author James Myall wrote: “I don’t think that it’s impossible for the state to do this, at least from an economic standpoint.” Myall said that Maine residents would save money, despite any new taxes, because care would be virtually free. Moreover, without the need to pay premiums, deductibles or copays, at least 85-90% of families would thus come out ahead and have more cash to spend. Furthermore, businesses would be unburdened from the cost of employee health insurance. Crucially, no person would be uninsured during a pandemic or economic crisis.
Maine Healthcare Action, a nonprofit 501(c)(4) organization started by local Maine physicians and concerned residents, has launched a campaign to put direct pressure on our Legislature in the form of a citizens-initiated resolve. The resolve directs the Legislature “to develop legislation to establish a system of universal healthcare coverage in the State and directs the joint standing committee to report out a bill to the Legislature to implement its proposal by 2024.”
We have begun to collect petition signatures to approve the resolve that will be presented to Maine voters in November 2022. The resolve is simple and straightforward, reflecting the will of the electorate that our Legislature address the inequities and costs of a dysfunctional delivery system and pass comprehensive healthcare reform. Any legislation should be tailored to the needs of Maine residents, and unlike today’s “take it or leave it” insurance-based system, the Legislature could guarantee health care, not just “coverage.”
Universal healthcare — everyone in, no one out — creates unity and solidarity: foundational aspects of American democracy.
William Clark, MD, of Brunswick is a board member with Maine Healthcare Action. Larry Kaplan, MD, MPA, of Cape Elizabeth is the organization’s chairman.