A national health advocacy group is blaming hospital consolidation in
Maine for spurring higher prices at hospitals for patients with private
insurance.
But Maine hospital officials say consolidation is not the force
driving the prices, and that the explanation lies with the state’s older
population and low Medicare reimbursement rates that shift the costs of
health care to younger people with private insurance.
Maine’s two biggest hospital systems – MaineHealth and Northern Light
Health – have both grown larger over the last 20 years, with formerly
independent hospitals joining their networks.
Mid-Coast Hospital in Brunswick and the former Goodall Hospital
in Sanford are among the more recent additions to the MaineHealth
system, which includes Maine Medical Center in Portland. Mercy Hospital
in Portland and Mayo Regional Hospital in Dover-Foxcroft are among the
hospitals that in recent years joined Northern Light Health, which
includes Eastern Maine Medical Center in Bangor.
While independent hospitals and other networks remain – including
Central Maine Healthcare in Lewiston and MaineGeneral Medical Center in
Augusta – MaineHealth and Northern Light dominate the state’s health
care market.
“What causes prices to rise uncontrollably, leaving patients subject to thousands
of dollars in medical bills? Look no further than consolidation, where
dominant hospital systems control markets and set prices as high as
they’d like,” said Darbin Wofford, health policy adviser for Third Way, a
center-left think tank based in Washington, D.C. Health care reforms
are among the topics that Third Way advocates for, including clean
energy, reforming gun laws and abortion access, among many other issues.
Third Way is releasing a case study analysis of Maine’s hospital
costs on Thursday and provided the Press Herald with an early look at
the findings.
In an interview, Wofford said consolidation in states such as Maine
tips the scales heavily in favor of hospital networks when negotiating
contracts with insurance companies. Those contracts influence the health
insurance premiums, deductibles and other costs that people pay.
“Insurance companies can’t say to hospitals, ‘No, we don’t want to take your prices,’ ” Wofford said.
According to the Health Care Cost Institute, the Portland market was
the 21st “most concentrated” health care market of 183 markets measured,
which means Portland has less hospital choice for patients than much of
the country. The Portland market was the only market measured in Maine.
Wofford pointed to hospital prices for private insurers, which are on
average 275% of the prices Medicare pays for services, or nearly three
times as high. Maine’s average costs are the highest in New England, and
far above the national average of 224% of Medicare, it found. Maine’s
average costs rank 19th among states. South Carolina is the state with
the highest hospital prices for private insurers, at 322% of Medicare
prices.
But Dr. Andy Mueller, CEO of MaineHealth, said the explanation for
private insurance prices at hospitals has far more to do with Maine’s
demographics.
When a higher percentage of the hospital patient mix is insured by
Medicare – generally patients 65 and older – that skews hospital prices.
Because Medicare’s reimbursements are so low and do not cover
hospitals’ actual costs, the difference has to be made up by private
insurers, Mueller said.
That’s true of any hospital in the country. But, he said, “we’re the oldest state in the nation.”
OLDEST STATE IN THE NATION
According to the U.S. Census, Maine’s median age is 44.8 years, the
oldest in the nation. “That puts a greater burden on those who have
commercial insurance to make up the difference,” Mueller said.
Terri Canaan, chief marketing and communications officer for
MaineHealth, pointed to an analysis that showed Maine’s Medicare
spending per enrollee – which includes hospital and non-hospital
spending – is below the national average. The national average is
$11,080, while Maine’s spending is $9,159 per enrollee, according to
KFF, a national health policy think tank.
Health care costs are influenced by a number of factors, such as the
push and pull of health care network contract negotiations with
insurers, the health and demographics of the population served, federal
and state regulations, and competition among health care providers,
among other things.
A Forbes Advisor analysis in 2022 combined 11 key health care cost
metrics to try to determine the difference in health care costs by
state. By that measurement, Maine has the seventh-highest health care
costs in the nation, at $11,505 per person. South Dakota was the most
costly in the nation, with $11,736 per capita, while Michigan had the
lowest health care costs at $9,524. The analysis includes all health
care costs, not just the costs incurred at hospitals or costs paid with
private insurance.
Denise McDonough, president of Anthem Blue Cross and Blue Shield in
Maine, said hospital consolidation is one of the factors driving up
costs in Maine.
“We have seen significant hospital consolidation in Maine over the
years, which has reduced competition, increased costs, and limited
access to care – leaving Mainers with less choice,” McDonough said.
Anthem and MaineHealth became embroiled in a public contract dispute
in 2022, with Maine Medical Center nearly withdrawing from Anthem’s
network in 2023 before an agreement was reached in August 2022. The
dispute became public with both sides providing the media with examples
of hospital overcharging of patients, and of the insurance company
denying needed care.
Both Anthem and MaineHealth officials have claimed that the other side has too much leverage in negotiations.
Mueller, on Wednesday, countered the argument made by Third Way that Maine’s hospitals have leverage over insurers.
“We’re still a ‘mom and pop’ industry in comparison to the
consolidation that has happened on the health insurance side,” Mueller
said. “These are massive companies, and we are not, relative to
(insurers). We are a tiny speck on the wall compared to them.”
REFORMS PROPOSED
Third Way has proposed a number of reforms, including tougher price
transparency laws, and laws that they say would help insurers when
negotiating with hospital systems.
Maine is debating regulation of facility fees, which can reach
hundreds of dollars for patients for just walking into a hospital for
care and are often hidden in medical bills and passed onto the patients.
After a Press Herald report in 2022 that featured patients complaining
about facility fees, the Maine Legislature passed a bill that created a
task force, which is studying possible changes to state law.
The federal government requires hospitals to disclose prices, but
some say the law doesn’t go far enough and lacks an enforcement
mechanism. Maine has the CompareMaine.org website, which allows for
comparison pricing of some procedures, such as colonoscopies, blood
tests and hip replacements.
McDonough, the Anthem president, agrees that more needs to be done, and calls Third Way’s suggestions a “good first step.”
But Mueller, the MaineHealth CEO, said that one of the bills
currently under consideration by the Maine Legislature would protect
insurers’ ability to reduce costs, such as by giving financial
incentives to patients to go to less expensive clinics. MaineHealth does
not prevent such cost-saving efforts, he said.
But Mueller said also built into the bill – L.D. 1708 – is a
provision that would prevent hospital networks from terminating
contracts with insurers.
“The only leverage we have is to terminate a contract,” Mueller said.
“We believe we ought to have the ability to terminate an agreement the
other party is not living up to.”
McDonough said, “we hope we can continue the conversation about
greater transparency and advance legislation to protect members’ access
to affordable care.”
https://www.pressherald.com/2024/01/04/national-advocacy-group-blames-hospital-consolidation-for-maines-high-health-care-costs/
Opinion: Physicians like me know our health care system must change
A recent experience as a patient served as a good example of how dysfunctional things can get.
by Scott Schiff-Slater - Portland Press Herald - January 4, 2023
I am a physician with a small family practice in Central Maine, and I love my job.
Our health care system in the U.S. is amazing, and yet it is also
dysfunctional, expensive, inefficient and needs to be changed. Let me
offer an illustration.
About a month ago at a Maine hospital I had a new type of scan done
that can spare people like me from invasive cardiology procedures. That
is the great part.
The bad part is that although I have excellent health insurance, and
the procedure was fully approved, my out-of-pocket expense was $1,029.84
– well above my $180 co-payment. The reason, I learned, is that I was
given one dose of nitroglycerin – we all know what nitroglycerin is,
people with angina keep it in their pockets – but this was part of the
protocol for the test as it is used to dilate the coronary arteries. If
nitroglycerin is purchased at a pharmacy, insurance will cover it. If
you don’t have insurance at all, it might be a few dollars. The hospital
charge, my out-of-pocket expense for this one dose of nitroglycerin,
was $849.84.
I was taken aback, as a consumer and as a physician. After a number
of hours of research and many phone calls, I learned that it was
considered a “self-administered” medication, so not covered by insurance
while in the hospital. The reasons for the charge of $849.84 has to do
with our health care system and how it functions, or doesn’t. I want to
emphasize that the hospital was just doing what all hospitals in the
United States do as they struggle to make ends meet in our current
system.
I am hoping to reverse this charge. I’m working with hospital and
insurance company employees, all of whom are getting paid for their
time, while I do this on my own time. I am a physician who knows the
system and can make the appeal. For many Maine families, pursuing the
appeal would be challenging and the charge could break the family
budget. This is just one example of a problem in our health care system
and I know that many readers have similar tales – I hear about them
daily from my patients.
We have some of the best care and yet some of the worst. The United
States is by far the most expensive health care system in the world and
yet we have health outcomes for this investment that are embarrassing.
As a society, we must respond.
The Maine Medical Association is a professional organization of more
than 4,000 Maine physicians, residents and medical students and almost
all our members believe that our current health care system does not
meet our needs and requires comprehensive change. We do not all agree on
how to fix the system, just that it needs to be fixed.
The association has issued a revised statement on reform of the U.S.
health care system that reviews the problems we face and offers some
principles for change. It is not perfect, but I promise it will make you
think. I encourage you to read the statement on the MMA website: www.mainemed.com.
Maine physicians, MMA members and members of other physician
organizations urge change. Change can’t happen without more
understanding from everyone of the problems, and the potential
solutions, and then we’ll need help from our elected officials.
In the meantime, my heart test was OK. I will keep working on fixing that $849.84 charge.
https://www.pressherald.com/2024/01/04/opinion-physicians-like-me-know-our-health-care-system-must-change/
Hidden charges, denied claims: Medical bills leave patients confused, frustrated, helpless
by Joe Lawlor - Portland Press Herald - January 12, 2023
Bill Bartlett received an $813 bill for a routine cardiac stress test
that he had been told would cost him $45. Sean Dundon was charged $800
for having his sliced thumb examined and bandaged.
Both patients faced unexpectedly huge expenses for simple medical
care because so-called “facility fees” were tacked onto their bills. The
fees are just one example of the arcane and complex world of medical
billing that so often frustrates and confuses patients.
Patients receive bills bloated by health care providers that
overcharge for services and insurance companies that deny claims without
explanation. And with little clout to fight back or even negotiate,
feeling helpless, they often give up and pay, worn down by a system that
is as time-consuming as it is obtuse.
A public, high-stakes battle between Maine’s largest hospital and its
dominant insurance carrier has opened a window into the opaque world of
medical billing and insurance claims, and it underscores just how
powerless consumers are.
The dispute was settled last week, but the disagreement was over
money. Maine Medical Center in Portland said Anthem owes it millions of
dollars in overdue and unpaid claims, while Anthem contended that Maine
Med has overcharged the insurer by millions of dollars. If the standoff
had not been resolved, Maine Med would have left Anthem’s provider
network in January, upending Maine’s entire health insurance market.
The Portland Press Herald/Maine Sunday Telegram spent more than three
months investigating the byzantine system of medical billing in Maine.
The newspaper spoke with dozens of patients who have had billing
problems, reviewed their invoices and explanations of benefits,
interviewed health care executives and consulted experts in the field.
The reporting reveals systemic shortcomings that are not limited to any
one medical provider or insurer but are pervasive across the landscape.
The Press Herald found that:
• Medical bills are confusing and opaque, and
sometimes carry arbitrary and hidden costs, including a common surcharge
that hospitals call a “facility fee,” charging hundreds of dollars
simply for getting treatment in a hospital.
• Insurance companies deny some claims for reasons
that aren’t clear and may never be explained, forcing patients to choose
between waging drawn-out fights or paying hefty bills.
• Costs for procedures and insurance coverage vary
so widely that even patients who carefully compare prices beforehand can
wind up with bills far larger than expected.
• Even though Americans’ access to insurance
expanded through the Affordable Care Act, many are still underinsured
and subject to massive medical bills they don’t expect and may not be
able to pay.
The practice of assessing facility fees – sometimes hiding such fees
in other charges – increasingly contributes to some patients’
surprisingly large bills.
It has long been standard practice for hospitals to shift
uncompensated costs, such as care for uninsured patients who can’t
afford to pay their bills, to patients with insurance.
But with more patients on high-deductible plans – and insurers
sometimes refusing to pay or paying only a fraction of their bills –
individuals are picking up more of the tab and bearing more of the
financial burden.
“The system is broken and is really in need of a major overhaul,”
said Dr. Julie Keller Pease, a founding member of Maine AllCare, which
advocates for single-payer systems like those in Canada and the United
Kingdom.
Still, any efforts to reform or overhaul the system, especially in one small state like Maine, face huge barriers.
HIDDEN FEES
Maine patients are paying hundreds of dollars extra for routine
medical tests or procedures simply because the tests are occurring at
hospitals. And they may have no idea, because the “facility fees” are
not clearly explained and sometimes hidden on their bills.
Bill Bartlett of Kennebunkport said he called his insurance company
to check on the price before getting his routine cardiac stress test
last November. A few weeks later, the 60-year-old got a bill from York
Hospital for the $45 he expected plus $813 for a “facility fee.”
Bartlett only discovered the facility fee because he demanded an
explanation. And before he spent months complaining and appealing, his insurance company tried to deny coverage and stick him with the bill.
“This shouldn’t be my problem,” said Bartlett, who appealed the
denial. “I did due diligence to determine the cost ahead of time.”
After Bartlett refused for months to pay the bill, Harvard Pilgrim finally paid most of it a few weeks ago, without explanation.
Jean Kolak, a spokeswoman for York Hospital, said that “when a
patient receives services at York Hospital, their invoice will include a
facility fee.”
“The amount of this fee is created, based on a variety of factors,
such as the cost of staff, equipment, technology, medications utilized,
supplies and in some clinical care areas, the acuity of the patient,”
Kolak said in a statement.
Ann Woloson, executive director of Consumers for Affordable Health
Care, a Maine-based advocacy group, said the organization is receiving
increasing numbers of complaints about facility fees and may seek
legislation to limit when they can be charged and require that patients
be warned ahead of time.
“If facility fees are charged, the brunt of those fees should not be on the consumer,” Woloson said.
Al Swallow, chief financial officer for MaineHealth, the hospital
network that includes Maine Medical Center and seven other Maine
hospitals, said facility fees are an industry standard. They reflect
the need for hospitals to cover higher expenses than other medical
providers incur, he said.
“Hospital settings have more costs than (outpatient) settings,
including the fact that many of the services delivered by hospitals go
uncompensated, either because of charitable care or the fact that
Medicare and Medicaid do not cover the full cost of care delivered in a
hospital,” Swallow said in an email response to questions. “Hospital
settings are also more highly regulated, and meeting those standards can
add costs to delivering care in those settings.”
DENIED CLAIMS
Patients can be at the mercy of insurance companies that deny claims
for services they thought would be covered, and some fight their bills
for years, believing that they should not be responsible.
Others just give up and pay, even though they share that belief.
Doni Gallinger of Portland did not give up, despite having claims
denied by two insurance companies. But it took years for the 70-year-old
to get coverage for mental health therapy.
“There was a very clear intent … to withhold services,” Gallinger said. “That was a very clear objective for them.”
The system is a perplexing mess, even for health care professionals.
Jill Copeland, a mental health therapist in Yarmouth, said she had to
learn the ins and outs of how seven insurance companies conduct
business in order to get properly reimbursed. If she didn’t have to
spend so much time navigating the system, she said she could see 15% to
20% more patients.
“I have waited a very long time to get paid,” Copeland said. “And I am very persistent.”
Getting insurance companies to fix problems related to reimbursements is often difficult.
“My experience has been in general if they get things set up right
the first time, it’s likely to keep going right,” Copeland said. “But if
something doesn’t go right the first time, it feels like you might as
well just give up. You can spend hours and hours and hours on the phone
and be given all kinds of promises that it’s fixed and then it still
isn’t fixed.”
UNPREDICTABLE PRICES
Patients trying to navigate the health care market find dramatically
different prices among medical providers. Many learn the hard way.
In 2021, Alex St. Hilaire of Westbrook got a CT scan on his abdomen
at Shields Imaging Center in Brunswick; it cost about $750. The next
year he had the same exact scan at Northern Light Mercy Hospital – and
it cost him nearly $3,000. With a high-deductible insurance plan,
Hilaire is on the hook to pay most of that total. He had no idea charges
for the same service could vary so much.
“I was literally in the machine 40 seconds tops, and it cost $3,000,” St. Hilaire said.
High charges are sometimes the result of a hospital rolling in other
costs and services, said Christy Jolliff, Northern Light Health’s vice
president of enterprise revenue cycle, who was speaking generally, not
about St. Hilaire’s bill. If a bill shows $25 for a bottle of aspirin,
that fee may actually cover other materials and services.
“We don’t charge for every piece of gauze, every Q-tip that’s being
used,” Jolliff said. “Oftentimes, it covers things that don’t get listed
at all.”
Why do hospitals charge so much? “Because they can,” said Jim Ward,
president and principal of Patient Advocates, a Gray company that works
with self-insured employers to lower health care costs.
Large organizations and insurance networks have the power to negotiate with hospitals, Ward said. Individual patients don’t.
Unlike neighborhood restaurants, hospitals generally don’t compete
for business with customers. Rather, they are looking to cover many
running costs.
“Hospital pricing is not the same as pricing for goods in a retail
store in that it is not done looking strictly at what other providers
charge,” said Swallow, the MaineHealth executive. “Rather, hospitals
start with the premise that they must cover their operating costs –
including free care and costs not fully covered by Medicare and Medicaid
– and leave enough of an operating margin to weather future adverse
events and invest in new technology and infrastructure.”
SHOPPING AROUND
There are ways to reduce the odds of an unexpected bill, but they don’t offer perfect protection.
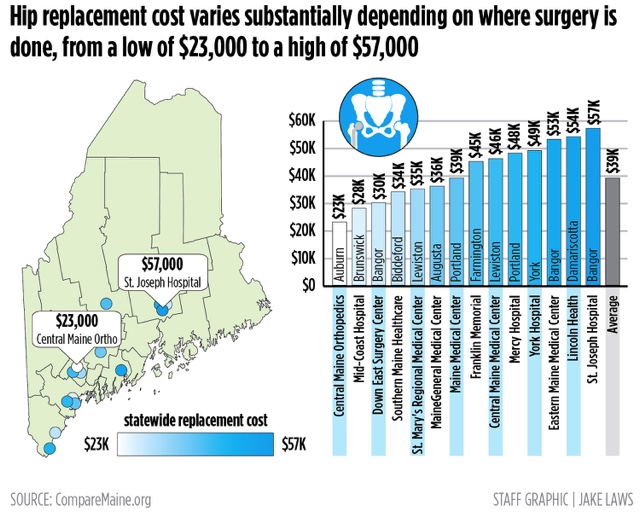
The state’s seven-year-old CompareMaine
website, launched by the Maine Health Data Organization, a state
agency, allows patients to compare the costs of procedures like a
colonoscopy or a knee replacement. The site reveals widely varying costs
across the state – a hip replacement can cost anywhere from $23,000 to
$57,000.
But the site doesn’t tell patients what facilities are in network for
their insurance companies – information that can dramatically affect
their share of costs. And it doesn’t help patients understand how to
navigate their coverage plans to control costs. It won’t tell you, for
example, that it is sometimes better for patients to meet their annual
deductibles before scheduling elective surgery.
In
an effort to increase price transparency, the federal government has
mandated that hospitals publish the “chargemaster” prices, or list
prices, on their websites.
But the chargemaster prices often have little to do with what
patients get charged. The list price of repairing a broken wrist may be
far different than what the various insurance companies, negotiating
with hospitals, have agreed to pay for that surgery.
The bill a patient receives in the mail may be a full three steps removed from the chargemaster prices.
Stephanie DuBois, a spokeswoman for Anthem, said the company
encourages its patients to shop around for health care services and call
to find out what Anthem will pay.
“We all know a hospital setting can be one of the most expensive
places to receive care, which is why at Anthem Blue Cross and Blue
Shield we invest a lot of time and resources into educating consumers
about the various choices they have available to them,” DuBois said in a
written statement. “Services such as imaging, labs, or prescription
drug infusion are available at many non-hospital based facilities that
offer consumers a convenient location, a much lower cost, and equal, if
not greater, quality.”
INSURANCE GAPS PERSIST
More Americans have health insurance now than ever before because of
the Affordable Care Act, which took effect in 2013. Still, about 8
percent of Mainers remain uninsured. And many others are underinsured,
with high deductibles or cost-sharing arrangements that shift more of
the financial burden onto them.
The proliferation of high-deductible health plans – designed to keep
premiums down – means patients are paying a higher share of the bills
that come in when they get sick.
While medical bankruptcy is rarer than before the ACA took effect,
many patients are saddled with thousands of dollars in bills that they
are unable to pay.
Valerie
Lawson, 65, of Calais said she was shocked by the $20,000 bill she
received when she was temporarily uninsured last winter. She had
dropped her insurance because the premiums were so high, and during that
lapse she had to go to the emergency room because of hemorrhaging in
her colon.
She learned what she owed when she was still weak and recovering at
home. “I felt like the floor opened up beneath me, and I fell through,”
she said. “I thought, ‘You have to be kidding me.’ I was really
gobsmacked.”
Lawson said she gave up fighting what she believed were unfair
charges and paid $14,000 to settle the bill because the fight took too
much energy, and being uninsured she was in a poor negotiating position
with Northern Light Eastern Maine Medical Center. She is now insured
again.
But it’s not only people without insurance getting large bills.
People who are underinsured – often with high-deductible health plans to
keep monthly premium costs low – end up paying high-cost bills.
The large number of underinsured people does more than land them with
massive bills. It also contributes to inefficiencies in the health care
system. The higher costs can make people reluctant to use their health
care plans, delaying health services even when they need care, experts
say.
“We focus on spending a lot of money later in the development of
disease, when we should be focusing on prevention, early diagnosis and
treatment,” said Reggie Williams, vice president of the International
Health Policy and Practice Innovations program at the Commonwealth Fund,
a foundation in New York City that supports health care reforms.
That increases the overall cost of health care and leads to worse
health outcomes, such as higher rates of infant and maternal mortality,
Williams said.
“The lack of investment we have in the United States before people
give birth really impacts the quality of care people have while they are
pregnant and postpartum,” Williams said.
REFORMS RESISTED
At the root of the problem is the way health care is financed in the
United States. It is a system that is hard to defend, even for hospital
administrators and insurance executives.
Yet it persists.
MaineHealth’s president, Dr. Andy Mueller, said the system needs to
change, and he wants to enact meaningful reforms that would move payment
models away from charging fees for services to paying health care
providers for keeping people healthy. Mueller said the financial
incentives need to move from volume charging for services to prevention
and management of chronic conditions, early diagnosis and treatment – in
other words, keeping people out of the hospital.
“We can’t accept the status quo,” said Mueller, who became the leader
of Maine’s largest hospital network in 2021. “We need to fundamentally
change the way we get paid.”
Mueller agreed that massive reforms would be daunting. But he said
MaineHealth expects to launch some pilot programs later this year that
could begin to make a difference. Details of the programs – which will
require a waiver from the federal Medicaid program – will be released
this fall.
“Rest assured, we are working on lots of reforms that will change how
we deliver care while increasing affordability,” Mueller said.
But Jim Ward, the Patient Advocates president, said the headwinds against meaningful change are strong.
Any change has the potential to benefit one sector of the industry at
the expense of another, and would face powerful resistance. “There’s a
very strong established and vested interest in maintaining the status
quo,” Ward said.
Some see the solution in a single-payer system – where the government pays for medical care, financed through taxes, eliminating
much of the market for insurance companies. It would force hospital
networks and other medical providers to accept prices set by the
government – as they do with Medicare and Medicaid.
Other countries, such as Canada, the United Kingdom, France and
Spain, and much of the developed world, have instituted single-payer
systems or universal coverage.
Liberal politicians and advocates in the United States, such as Sen.
Bernie Sanders of Vermont, have long called for a single-payer model,
which Sanders describes as “Medicare for all.” Conservatives have
opposed the idea, calling it socialized medicine.
Other substantial but less sweeping reforms that are often discussed
include lowering the age eligibility for Medicare from 65 to 55 or 50
and giving people a “public option” for health insurance. But action on
such fronts does not seem to be on the horizon, and much narrower
changes are hard fought.
Even a modest reform that attracted bipartisan support – letting
Medicare negotiate prices with drug manufacturers – took decades of
advocacy. The Medicare reform, which finally cleared Congress and was
signed into law by President Biden last week as part of the Inflation
Reduction Act, will also limit annual out-of-pocket prescription costs
for Medicare patients to $2,000.
A proposal championed by U.S. Sen. Susan Collins, R-Maine, would have
capped insulin copays at $35 per month. The Inflation Reduction Act
that passed Congress included this copay limit for Medicare patients,
but not for the rest of the population. Collins and other advocates hope
to bring forward a separate bill to pass a broader insulin cap.
Woloson, executive director of Consumers for Affordable Health Care,
said it’s difficult to enact reforms that benefit patients given the
competing interests of the major players in the market, such as
hospitals, insurance companies and drug manufacturers.
“When you adjust something over here, you have to adjust over there,”
Woloson said. “The consumer is always left holding the bag. What works
best for hospitals or insurance companies might not work for patients.”
Some have tried to reform the system at the state level.
Massachusetts launched a system that sharply reduced the rates of the
uninsured and inspired the federal Affordable Care Act. In recent years,
the state established a health care cost commission, but it has little
regulatory power.
Maryland has worked for decades to regulate costs and reduce
incentives to over-treat patients. The state regulates and sets hospital
prices and places all the hospitals under a single “global budget,”
which means the finances for hospitals in Maryland are all lumped into
one budget.
But Maryland’s efforts have yielded mixed results, according to recent studies.
Woloson said such efforts are important incremental steps, but they
don’t represent substantial progress. “They’re not there yet,” she said.
Maine continues to study the feasibility of reforms. Last year, the
state approved the Office of Affordable Health Care, which is studying a
number of reform possibilities, including allowing people to “buy”
Medicaid coverage, expanding Medicaid and the Children’s Health
Insurance Program and further increasing subsidies for ACA plans using
state dollars.
The reforms, like the Affordable Care Act, tend to focus on expanding
access to insurance rather than addressing problems with pricing and
out-of-pocket costs.
SINGLE-PAYER A TOUGH SELL
Pease, of Maine AllCare, the advocate for single-payer systems, said anything short of single-payer will always be lacking.
“In single-payer systems like Canada, the doctor sends off the bill
for services to the government, and they get paid a few days or few
weeks later,” Pease said. “It’s very automatic and removes
inefficiencies. Insurance companies just add another layer of
bureaucracy, denying payments, requiring prior approval of services.
They’re the middleman.”
But no state has enacted a single-payer system, and the political
climate does not appear conducive to a national single-payer system.
Proposals in recent years to establish single-payer in Maine have
stalled out on numerous occasions.
Vermont came close in the early 2010s, but ultimately abandoned it
over the complexity of a small state going it alone and the difficulties
in a state financing the system.
California is considering a single-payer system, but a bill to create
one failed to get a vote in the state assembly this February.
Single-payer also may not be a panacea.
Mueller, the MaineHealth CEO, said that a single-payer system would
not necessarily be an improvement. If the government did not put enough
money into the system, there could be massive cuts to health care
services.
The way it is now, if there are cuts in government-funded Medicare and Medicaid, health care systems have the flexibility to make up for lost revenue by increasing costs to private insurers.
Health care systems would potentially lose that ability under a single-payer system, Mueller said. So,
if public funding for a single-payer system was insufficient or
inconsistent, it could result in cost-cutting and ultimately a declining
quality of health care, he said.
Dan Colacino, vice president of the Maine Association of Health
Underwriters, which represents brokers that sell insurance, said the
success of a single-payer system would be subject to the push and pull
of state budget negotiations.
“It moves the cost of health care from individuals and employers onto
the state,” Colacino said. “The increase in taxes would be huge.”
Without meaningful change, Maine patients are largely left to
navigate the medical billing maze on their own, learning one painful
lesson at a time.
Sean Dundon’s teaching moment came on Christmas Day, when he sliced
off a portion of his thumb peeling potatoes. The trip to Northern Light
Mercy Hospital for an assessment and a bandage – he didn’t even need
stitches – cost him about $300 for the actual treatment and another $500
for a hospital facility fee he had to use his deductible to pay.
Dundon said the system is “intentionally obfuscating and confusing”
and it shouldn’t be. “If there had been a sign on the wall that said
there was a facility fee, I would have gone home, dressed it myself and
gone (somewhere else) the next day.”
https://www.pressherald.com/2022/08/21/hidden-charges-denied-claims-medical-bills-leave-patients-confused-frustrated-helpless/
In their own words: Nine Mainers talk about their medical billing nightmares
Joe Lawlor - Portland Press Herald - April 27, 2023
To get a clearer understanding of the medical billing frustrations
that affect so many people, we invited readers to share their billing
and insurance problems with us. More than 100 people did. Here are nine
of their stories.
BRIAN AND EVELYN ROACH
Evelyn Roach of Gray gave birth to her first child in October.
Eamon was born six weeks premature and needed to stay in Maine
Medical Center’s neonatal intensive care unit for about two months.
While he’s now healthy and at home, Roach and her husband, Brian, spent
months fearing they would wind up hundreds of thousands of dollars in
debt for their new baby’s medical care.
The couple brought Eamon home Dec. 31. They had set aside money for
the pregnancy and birth because they have a high-deductible insurance
plan and expected out-of-pocket costs totaling a few thousand dollars.
But shortly after bringing the baby home, the couple got letters from
her insurance company stating their claims were denied and that they
would be on the hook for the full cost of his care: $360,000.
She and her husband made numerous calls to Anthem and MaineHealth,
the parent organization of Maine Med. She said they never got a clear
answer about why the claim was denied.
“It’s a massive amount of money. It’s almost incomprehensible,” Brian
Roach said while still trying to get answers in May. “How would we go
about paying for this?”
“No one (ever) said this is wrong and you won’t be charged for it,” Evelyn Roach said.
Finally, in June they got a bill from Anthem in Maine showing they
didn’t owe any money. They had already met their out-of-pocket
deductible of $6,600 earlier in 2021.
“We were so relieved,” Evelyn Roach said shortly after receiving the
news. “It was adding unnecessary stress to an already stressful
situation.”
But they still do not know why the claim was initially denied.
“It’s unclear to me what happened,” Evelyn Roach said. “Whenever I
spoke with someone, they were always kind and trying to be helpful, but I
could tell no one really could tell me what was going on.”
She said they notified the insurance within a week of Eamon being
born that he was being added to her insurance policy, meeting that
insurance requirement.
Evelyn and Brian have different insurance policies through their
employers, so they think this may have been an effort by Anthem of Maine
– Evelyn’s policy – to get Anthem of Illinois – Brian’s insurance
coverage – to cover the birth. But no one has confirmed that.
Evelyn Roach said the experience made her feel helpless.
“Eamon needed to be in the hospital after he was born, and we
shouldn’t have had this hanging over our heads,” she said. “Why was this
so stressful and confusing?”
ALEX ST. HILAIRE
Alex St. Hilaire needed a CT scan twice in the past two years for abdominal pain he was experiencing.
The tests were identical. In both cases the 31-year-old’s symptoms
turned out to be false alarms. But the two bills he received were
starkly different.
In February 2021, St. Hilaire went to Shields Imaging in Brunswick
for a CT scan and ended up with a bill of $742. Because he has a
high-deductible health insurance plan, St. Hilaire knew he was going to
pay the bulk of the cost, and the bill was in the ballpark of what he
was expecting.
In February 2022, the Westbrook resident needed another scan. He was
having difficulty scheduling one, so he asked his doctor’s office to
give him other places to try. He was referred to Northern Light Mercy
Hospital in Portland, where he went for the same CT abdominal scan
conducted at Shields Imaging the previous year.
The cost: $2,900.
“I was expecting $600 to $700. I was not expecting $3,000,” St.
Hilaire said. With the high-deductible plan, he was on the hook for most
of the money, although he was able to get a discount to $2,500 by
immediately paying in full.
All for a procedure that took less than five minutes.
“I remember the tech saying, ‘All right, done.’ I was literally in
the machine 40 seconds tops, and it cost $3,000,” St. Hilaire said. “It
didn’t ruin my year, but certainly I could have done something else with
that money.”
St. Hilaire said it doesn’t make any sense that the same procedure could have such wildly different costs.
It’s a painful lesson learned by countless health care consumers in
the U.S., where all kinds of medical costs vary widely for the same
procedures. In Maine, for example, a hip replacement can cost $30,000 in
one hospital and $60,000 in another.
“Why are we paying crazy bills like this?” he said.
ED LATHAM
When Ed Latham experienced chest pains in May, he checked himself
into Northern Light Maine Coast Hospital in Ellsworth for observation.
The 53-year-old had three previous heart attacks, so he relied upon
his cardiac surgeon’s “strong recommendation” that he be hospitalized
for observation and tests. Latham said he was concerned about whether
insurance would cover his six-day hospital stay, but he wasn’t going to
go against his doctor’s recommendation.
“I understand their thinking of it’s better to be safe than sorry,”
said Latham, who lives in Milbridge. “They didn’t want me walking out of
the hospital and dropping dead on the street a few blocks away.”
Latham’s heart was OK, and he was released. A few weeks later he got a
letter from his insurance company stating that the claim for his
hospital stay would be denied and not covered. There was no explanation.
After months of waiting, he received a few bills from the hospital
totaling hundreds of dollars, but Latham said he has no idea if he’s
getting more bills and could be on the hook for thousands in payments.
Latham said he called the hospital’s billing department, and they
told him that it will likely be worked out between the hospital and
Anthem, his insurance carrier. But in the meantime, the possibility that
he could owe thousands continues to weigh on him – he still has not
been told how much the bill could be.
“Why am I involved in this at all?” Latham said. “They shouldn’t be
putting me in the middle of a dispute between the hospital and the
insurance company about what is payable and not payable.”
Latham said the entire situation is alarming.
“The insurance company is essentially saying it is logical to go
against your doctor’s wishes for their financial considerations,” Latham
said.
DAVID SANBORN
Once a year David Sanborn of South Berwick gets an endoscopy for his
throat to make sure a pre-cancerous condition doesn’t return.
And every year he has to fight with his insurance company over the bill.
His medical provider is in the insurance company’s network, but his
doctor sends the biopsy to an out-of-network lab. His insurance company,
Cigna, has billed him for the entire cost of the lab work – $4,300 –
every year.
“Every single time it’s been a different problem, and every time they
are trying to stick me with a lab bill,” Sanborn said. “Their policies
are consistently changing. It’s aggravating. It’s a procedure I am going
to need next year and the year after that and for the rest of my life.
It should be paid.”
So far, the 46-year-old has been able to eventually get the cost
covered. But he said it’s infuriating to have to go through the hassle
every time.
Sanborn said he could have his doctor seek a different lab, but doesn’t want to compromise on his care.
“When my doctor decides this is the best lab to send the sample to,
I’m not inclined to argue with my doctor,” he said. “He’s the expert.”
DONI GALLINGER
Doni Gallinger fought for years with two insurance companies over coverage for mental health services.
When the 70-year-old enrolled in Medicare five years ago, she also
purchased insurance that provided supplemental coverage for mental
health. Gallinger said she was assured that her therapist – Jill
Copeland, a licensed clinical professional counselor – would be included
in her insurance plan.
Nevertheless, Gallinger said, the companies denied the claims.
“They just wouldn’t bloody do it. They just wouldn’t,” she said.
Gallinger said she ended up having to pay $1,500 out-of-pocket before
her mental health services were finally covered, but she spent many
hours on the phone and writing letters to get the service covered. The
hold-up was over the fact that standard Medicare does not reimburse for
counseling by an LCPC even though her supplemental insurance plan was
supposed to.
“The only answer I would ever get is that, ‘We won’t cover it because
Medicare doesn’t,'” said Gallinger, who wrote letters to Sen. Angus
King and to Rep. Chellie Pingree to put pressure on the insurance
companies. “There was a very clear intent … to withhold services. That
was a very clear objective for them.”
The only reason she eventually broke through and got it covered was
by being extremely persistent with letters and appeals. In one May 2019
letter to Aetna, Gallinger was so frustrated that she wrote: “(May) God
forgive you for harassing people with health problems, rather than
giving them the services they have contracted and paid for.”
Gallinger, who lives in Portland, said that in all the time she has
dealt with insurance companies, “they don’t ever seem to make mistakes
where there’s a benefit in your favor.”
She lived in Canada as a young woman and remembers learning about how
the U.S. system was so different from the simpler Canadian system,
which covers people without sending them into medical bankruptcy.
“When I was in Canada, we always watched in horror what was happening
in the U.S. (with the health care system),” Gallinger said. “We
wondered why they put up with it. The system is barbaric.”
SIMONNE MALINE
Simonne Maline has osteoarthritis in both knees. She uses walking
sticks to get around, and for more than a decade she has relied on
periodic injection treatments to keep the pain manageable and avoid
surgery.
Now, however, the 56-year-old is so far unable to get the same
treatment that has helped her in the past because it may not be covered
by her plan.
“It’s discouraging and frustrating and makes me angry that my life is
limited because of insurance and money,” said Maline, who lives in
Winthrop. “And it’s not even based on science. It boggles my mind. Life
shouldn’t have to be this hard to get care.”
Maline said her insurance company turned her down two years ago when
she requested SynVisc-One injections. She is being required to try
another treatment first before her doctor can request the SynVisc-One
injections again, and it’s not clear another request would succeed.
She fell on the concrete floor in her garage last fall, further
aggravating her left knee. The treatment injects a gel that lubricates
the knee. The company’s website says some insurance plans will cover the
procedure, while others won’t.
The cost of a SynVisc-One is about $1,000 to $2,000 plus the cost of a
health professional to give the injection. It’s far less than the
$30,000 or higher price of knee surgery, which she said she will likely
need if she can’t get the treatments.
The injections – which she has undergone three times in the past 15
or so years – have provided years of pain relief and mobility. But in
recent years insurance companies have balked at paying for the
treatments because it’s ineffective in some cases.
“I have a proven history of the treatments working for me, so this
should be the first line of defense for me,” said Maline, who happens to
be executive director of the nonprofit Consumer Council System of
Maine, which advocates for improvements in public policy for mental
health services.
Instead, she will have to try cortisone shots that, based on past
experience, she believes will not work. If the gel injections are not
approved after that, she will have to wait more than six months for knee
surgery.
And not only would a knee replacement surgery be more costly for the
system, but the recovery time from surgery would mean she could not care
for her husband, who uses a wheelchair and is disabled from a brain
injury. Knee surgery for Maline would mean her husband would need to go
to a nursing home.
Maline also has about $25,000 in medical debt as a breast cancer
survivor and needing three surgeries related to her cancer and other
medical problems. For three years in a row, she hit her $7,000
out-of-pocket maximum with her insurance plans. So even though she’s
insured, it’s put her into debt.
“When you look at what you have to pay out of pocket, it becomes a
huge financial burden that becomes insurmountable,” Maline said.
VALERIE LAWSON
Valerie Lawson said she knew she was rolling the dice in early 2021 when she chose to be without health insurance temporarily.
At age 64 and only a year away from qualifying for Medicare, she
could no longer afford to pay her health insurance premiums through the
Affordable Care Act. A few weeks later, the Biden administration
increased subsidies for middle-class people like Lawson nearing
retirement age, and she quickly signed back up.
But during the month that she was uninsured, Lawson experienced
hemorrhaging in her colon and had to be hospitalized at Northern Light
Eastern Maine Medical Center in Bangor. Her condition didn’t require
surgery, but the bill for a two-day hospital stay totaled $21,000.
“When I first heard the total amount on the phone, I felt like the
floor opened up beneath me, and I fell through. I thought, ‘You have to
be kidding me.’ I was really gobsmacked,” said Lawson, who lives in the
Washington County town of Robbinston.
So Lawson – still weak from her hospital stay – took it upon herself
to examine every aspect of her bill, to see what could be challenged.
“It was exhausting,” she said. “I was still quite ill. I couldn’t even stand up for 5 minutes at a time, I was so weak.”
She looked over the charges and found they were consistently higher
than the official “chargemaster” prices published on the hospital’s
website. The chargemaster prices are the initial price set by the
hospital, but they are often different than the charges negotiated with
individual insurance companies. In one case, an iron IV infusion to help
speed her recovery cost more than $3,000, when the chargemaster price
indicated it should have been only about $50.
“If I had known how much that was going to cost me, I would have
said, ‘No, thank you, I’ll have a steak at home,” Lawson said. She said
Northern Light never gave her a reason for the price.
The hospital offered her a 25 percent discount on the overall bill, which she took, and is now paying off about $14,000.
While Lawson now qualifies for Medicare – and with supplemental
insurance shouldn’t have to worry about getting socked with any more
giant bills – she said the money she spent means that she will have to
delay her retirement from her work in website design.
“You really go through the wringer when this happens,” Lawson said.
“It just grinds you down, just no way out of it. I eventually just gave
up.”
SEAN DUNDON
Christmas 2021 started painfully for Sean Dundon.
He was at home in Portland doing some morning food prep. “The first
slice of peeling potatoes, I sliced a portion of my finger off,” he
said.
Dundon, 54, said he wanted to make sure it wasn’t a serious injury,
so he went to the Northern Light Mercy Hospital Emergency Department in
Portland. He said he would have gone to an urgent care center but they
were all closed for the holiday.
“They gave me Lidocaine (anesthetic), cleaned out the wound, wrapped
it up and sent me home in half an hour,” Dundon said. He didn’t need
stitches.
“I came home and opened presents and thought, ‘This was great.'”
The bill arrived a few weeks later: $800, which included a $510
“facility fee” for using the hospital on top of about $300 in charges
for the assessment and treatment.
“If there had been a sign on the wall that said there was a facility
fee, I would have gone home, dressed it myself and gone (somewhere else)
the next day,” Dundon said.
A facility fee is charged by health care providers to cover the
expense of the overall services in the building, but insurance companies
will often pay only a fraction of the fee, leaving patients on the hook
for the bulk of the cost.
Dundon said he tried to appeal and negotiate a lower bill but was
unsuccessful. With a high-deductible insurance plan, he had to pay the
entire cost himself.
“They are basically admitting they are gouging me,” Dundon said. “It is intentionally obfuscating and confusing.”
BILL BARTLETT
Bill Bartlett’s doctor recommended he get a routine cardiac stress test.
So the 60-year-old from Kennebunkport called his insurance company in
advance to find out how much it would cost, giving them the name of the
York Hospital-affiliated doctor’s office to make sure it was in-network
and wouldn’t cost too much.
The answer: He would be responsible for $45.
It sounded reasonable, so Bartlett went for the test at York Hospital
in November. The test did not show any problems with his heart.
When he got the bill in February, it was for $858 – $45 for the
stress test plus $813 that was tacked on for reasons that weren’t
clearly explained.
When he asked what the $813 was for, Bartlett said his insurance
company, Harvard Pilgrim, told him it was a hospital facility fee, an
add-on because the test occurred in a hospital. And he was told the
insurance plan doesn’t cover most of the facility fee. The total
facility fee was $924. Harvard Pilgrim paid $111, and the $813 balance
was charged to Bartlett. After months of back-and-forth, Harvard Pilgrim
paid the bill, without explanation, in late July.
Bartlett said when he initially called to complain about the charge,
hospital officials were at first vague about the $813 but later
confirmed that it was a facility fee.
“When a patient receives services at York Hospital,
their invoice will include a facility fee,” said Jean Kolak, a
spokeswoman for York Hospital, in a statement to the Portland Press
Herald/Maine Sunday Telegram.
“The amount of this fee is created, based on a variety of factors,
such as the cost of staff, equipment, technology, medications utilized,
supplies and in some clinical care areas, the acuity of the patient,”
Kolak said. “Additionally, in cases where the physician/provider is
employed directly by York Hospital, a separate professional fee will also be charged.”
Kolak said the cost of the cardiac stress test and all other services
at the hospital are built into the facility fee, so it is incorrect to
say the stress test cost $45.
Bartlett said he thinks he should have been told about the total cost
when he called the insurance company to ask about the price.
“If I’m interested in buying a car, you don’t say, ‘How much are the
tires?’ No, you’re asking what the whole price of the car is,” Bartlett
said. “Harvard Pilgrim quoted me the price. Any additional costs are on
them (York Hospital).”
Kolak said “payments for services are based on contracted rates with
each payer” and that according to the contract with the insurance
companies, and in the case with Medicare or Medicaid patients “we cannot
waive patient responsibility” for charges.
The hospital offered to give him a payment plan, but Bartlett balked.
“Why should I go on a payment plan for something I don’t owe?” Bartlett said.
Bartlett refused to pay, and an initial appeal to Harvard Pilgrim was
rejected before being paid in late July without explanation.
“They have these charges that are invisible to consumers,” Bartlett
said. “This shouldn’t be my problem, I did my due diligence ahead of
time to determine the cost. It’s not like I have some exotic disease.
They should know what this is going to cost.”
Bartlett said that had he not been semi-retired and in good health, he may not have had the time and energy to fight the bill.
“I often wonder how many times medical providers send these bills
out, and get a check back because nobody’s going to argue or spend the
time to fight it?” Bartlett said.
https://www.pressherald.com/2022/08/21/in-their-own-words-nine-mainers-talk-about-their-medical-billing-nightmares
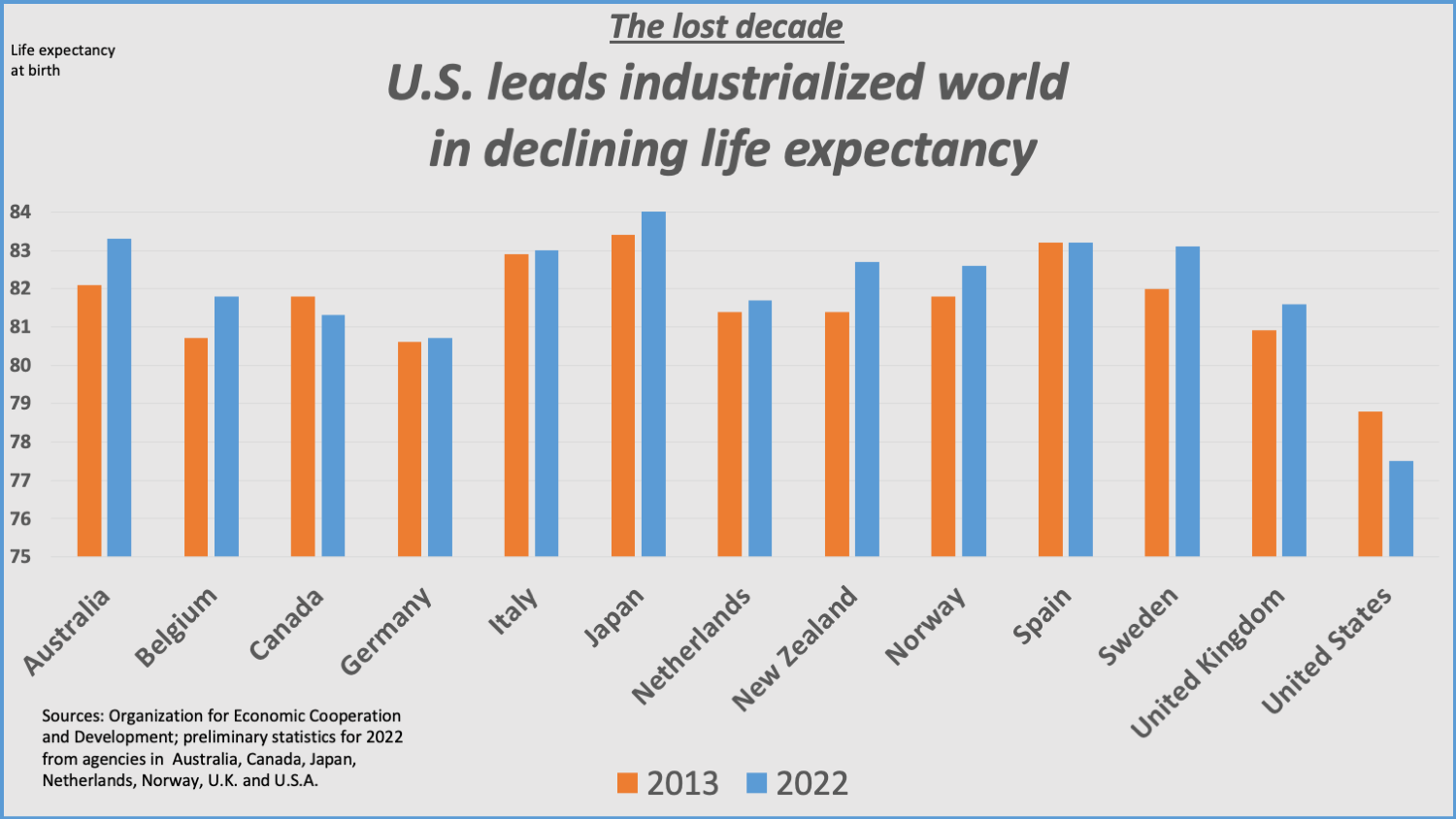
A
year after Califf’s dire warnings, Americans’ life expectancy decline
remains a pressing public health problem — but not a political priority.
President
Biden has not mentioned it in his remarks, according to a review of
public statements; his Republican challengers have scarcely invoked it,
either. In a survey of all 100 sitting senators, fewer than half
acknowledged it was a public health problem. While recent federal data
suggests that life expectancy ticked up
in 2022, a partial rebound from the ravages of the coronavirus
pandemic, no national strategy exists to reverse a years-long slide that
has left the United States trailing peers, such as Canada and Germany,
and rivals, such as China.
“I wish that
life expectancy or health span were a fundamental political issue in the
2024 presidential campaign,” said Dave A. Chokshi, a physician and
public health professor who formerly served as health commissioner of
New York. “We’re not living the healthiest lives that we possibly
could.”
The
Washington Post spoke with more than 100 public health experts,
lawmakers and senior health officials, including 29 across the past
three presidential administrations, who described the challenges of
attempting to turn around the nation’s declining life expectancy. Those
challenges include siloed operations that make it hard for public and
private-sector officials to coordinate their efforts, a health-care
payment system that does not reward preventive care and White House
turnover that can interrupt national strategies.
Many
suggested the nation needed an effort that would transcend political
administrations and inspire decades of commitment, with some comparing
the goal of improving life expectancy to the United States’ original
moonshot.
“We’re
no longer an America that talks about building a national highway
system or sending a man to the moon, and yet it’s that kind of reach and
ambition that we need to have to tackle the declining longevity
problem,” said Sen. Elizabeth Warren (D-Mass.).
Experts,
officials and lawmakers acknowledged that a political pledge to reverse
the nation’s life expectancy slide could quickly backfire, given the
need to focus on long-term goals that might not be reflected in
short-term progress reports. A politician attempting to improve life
expectancy could be out of office by the time improvements were
detected.
“Politicians,
in general, haven’t wanted to engage on this because it feels kind of
squishy and the solutions don’t seem clear,” said Ashish Jha, the dean
of Brown University’s public health school who this year stepped down as
the White House’s coordinator of the national covid response.
In
an interview, Califf confirmed he’d urged colleagues in “so many”
meetings to take action on America’s eroding life expectancy.
The
trend is “quite alarming,” the FDA commissioner said, sitting in his
office in White Oak, Md., where he oversees the nearly $7 billion agency
that regulates drugs, food and other common products used by
Americans. “All of the leaders within the [Department of Health and
Human Services] I’ve talked with about this.”
White
House officials said the president and his team were focused on
combating the “drivers” of life expectancy declines, pointing to efforts
to reduce drug overdoses, create an office to prevent gun violence
and other initiatives. A senior health official in the Biden
administration said pledging to improve life expectancy itself “would
have to be viewed as something for a legacy.”
“Maybe
a second-term priority for Biden,” said the official, who spoke on the
condition of anonymity to speak frankly about internal White House
operations.
The
paralysis over how to address the nation’s declining life expectancy
extends to Congress, where a handful of lawmakers — mostly Democrats —
have repeatedly portrayed the slide as a crisis, but most other
lawmakers have said little or nothing.
“We
don’t talk about life expectancy, because it just makes it clear what
kind of failed system we currently have,” said Sen. Bernie Sanders
(I-Vt.), who has repeatedly warned about the rise in premature deaths,
including organizing a July 2021 Senate hearing on the issue. Just 11 of
the panel’s 18 senators attended, several only briefly; just five asked
questions.
“I talk to other senators about life expectancy data and watch their eyes glaze over,” Warren said.
The
Post submitted questions about life expectancy to all 100 sitting
senators, sending emails, placing calls and making visits to their
offices. Forty-eight senators — including 35 Democrats, 11 Republicans
and two Independents — said they agreed that declining life expectancy
was a problem. Many of those lawmakers pointed to their own legislation
intended to combat opioid misuse and address conditions such as cancer
and other factors linked to causes of premature death. All told, the 48
senators cited more than 130 separate bills focused on health-care
issues.
Despite
the flurry of legislation, the nation’s progress on life expectancy has
stalled, with the United States increasingly falling behind other
nations well before the pandemic. No senator has crafted a bill
specifically intended to improve life expectancy or create goals for
health leaders to reach.
Lawmakers
have also worked at cross purposes, with Republicans fighting
Democrats’ efforts to enact legislation linked to gains in life
expectancy, including efforts to expand access to health coverage and
curb access to guns. Sen. John Neely Kennedy (R-La.), whose state had
the third-worst life expectancy in 2020, about 73 years, recently
suggested that life expectancy would even go up for young Americans.
“I
mean, the life expectancy of the average American right now is about 77
years old. For people who are in their 20s, their life expectancy will
probably be 85 to 90,” Kennedy said on “Fox News Sunday” in March. His
office did not respond to requests for comment.
Other
Republican senators or their staff suggested they did not have a view
on the issue because the senator did not sit on a relevant committee.
Sen.
Jerry Moran (R-Kan.) has “no jurisdiction over this issue,” his office
wrote in response to questions about whether Moran had views on
declining life expectancy. Moran, who sits on the Senate panel that
determines funding for health agencies, has cast votes on numerous
health-care matters, including repeatedly voting to repeal the
Affordable Care Act.
In
the absence of national solutions, some officials pointed to local
efforts such as a new initiative in New York, which has repeatedly
pioneered public health improvements later copied across the country.
City leaders in November pledged to raise New Yorkers’ life expectancy to a record 83 years,
saying a coordinated approach could prevent premature deaths. Ashwin
Vasan, the city’s health commissioner, testified in front of the city
council, urging members to pass a law requiring the city’s health
commissioner — including his successors — to work toward shared public
health goals.
“This
is a test for government. And I really am hopeful that New York City
can pass that test,” Vasan said after his testimony, standing outside
New York’s city hall.
“The
future of human longevity, especially for Americans, seems bright
indeed,” then-Sen. Larry Craig (R-Idaho) proclaimed at a 2003
congressional hearing, where expert witnesses listed scientific and
technological breakthroughs that they expected would soon push U.S. life
expectancy past 80 years.
But
even the most optimistic expert at the panel warned that America’s
prospects could dim. James Vaupel, director of the Max Planck Institute
for Demographic Research, urged federal officials to immediately
prioritize a “real mystery”: the emerging international gap in life
expectancy.
“The
United States is doing so well on so many fronts, but it’s falling
further and further behind on this critically important [measure], life
itself,” Vaupel warned the Senate panel, imploring officials to “really
start worrying about this.”
It
would take about a decade before Vaupel’s warning was heeded.
Policymakers instead were focused on a more urgent political priority
related to life expectancy: the growing cost of having so many older
Americans seeking services through programs such as Medicare and Social
Security.
So
when the Obama administration and congressional Democrats hammered out
legislation that would become the Affordable Care Act — the sweeping
2010 law that expanded health coverage to millions of Americans and made
other changes to the health system — there was little fear life
expectancy would decline.
Bob
Kocher, a venture capitalist who worked in the Obama White House as a
health-care and economic aide, said one reason the crafters of the
Affordable Care Act were so intent on “bending the curve” on health
spending “was our belief that life expectancy was going to keep going up
for the foreseeable future.”
By 2013,
public health experts had begun issuing more prominent warnings about
life expectancy, pointing to the rising number of opioid overdoses,
suicides and other preventable deaths. Senior officials across the
Obama, Trump and Biden administrations said they were aware of those
concerns but that their focus was on improving discrete factors linked
to life expectancy, not on the overall number.
“Every
meeting at the VA was about ‘life expectancy,’ but I can’t tell you we
put charts on the wall of ‘what’s the life expectancy of a veteran,’”
said Robert A. McDonald, secretary of veterans affairs under President
Barack Obama.
The
nation’s current top health official, Health and Human Services
Secretary Xavier Becerra, told The Post he’s acutely aware of the life
expectancy decline, calling it the “byproduct of some very serious
problems” such as gun violence and drug overdoses. But he downplayed the
need for a national strategy, saying there was no reason to
declare a public health emergency as he has done with the coronavirus
and opioid deaths, adding his agency lacked the power to reverse the
trend.
“We
are so disjointed as a health system in the country,” Becerra said,
suggesting that the responsibility to address life expectancy fell on
“many of us,” including state health directors.
While Biden hasn’t directly addressed declining life expectancy, some of his rivals have invoked it on the campaign trail.
“We
used to think that life expectancy was just going to keep going up, and
that’s just not been the case,” Florida Gov. Ron DeSantis (R) said in a
CNBC interview
in August, linking the decline to the pandemic, drug overdoses and
other causes that began years ago. The DeSantis campaign did not respond
to a request for comment about how the Florida governor would reverse
the trend if elected president.
“If
we had regulatory agencies that were actually interested in looking at
data, we would be trying to figure out why the all-cause mortality [for
Americans] has increased,” Robert F. Kennedy Jr., running as an
independent in the 2024 campaign, said in an interview with The Post
this summer. “These aren’t covid deaths.”
Political
commentator Matthew Yglesias has repeatedly urged politicians to focus
on life expectancy, saying that America’s decline reveals systemic
problems that leave the country at risk. “Tackling America’s weirdly short life expectancy should be a priority,” Yglesias wrote in one 2022 post.
Although
Yglesias has fans within the Biden administration who have sought his
counsel after he has written about traffic safety and crime, his appeals
on life expectancy haven’t led to similar invitations.
“I
think it winds up being a harder topic for politicians to get their
heads around,” he said, noting the array of factors that span agencies
and administrations.
Califf said he’s keenly aware of his agency’s limits when confronting life expectancy.
FDA
is one of the nation’s most powerful regulatory bodies — its staff
often tout that they oversee about 20 cents of every dollar spent by
U.S. consumers — and Califf is pursuing initiatives, such as banning menthol cigarettes
and improving access to generic drugs, that fall in his agency’s
purview. But FDA can’t control how hospitals and doctors get paid. It
can’t craft legislation, such as curbing access to firearms.
“The highest cause of death in children is guns. That’s a fact,” Califf said. “That’s not something FDA can do something about.”
In Congress, a handful of members have insisted that lawmakers must focus on life expectancy, saying it’s a core responsibility.
“Sometimes,
we may, in the midst of our work, lose sight of the big picture … to
create a nation in which the people in the United States can live long,
healthy, happy and productive life,” Sanders said at the 2021 Senate
hearing he convened on lagging life expectancy.
There
is a notable partisan split in how members of Congress view life
expectancy and whether they say urgent action is needed. Just 11 of the
Senate’s 49 Republicans told The Post they believed that declining life
expectancy was a public health problem.
The
lawmakers who portray the recent decline as a crisis are often
Democrats from states with the highest life expectancy — such as
Massachusetts (79 years in 2020, according to federal data) and Vermont
(78.8 years). Meanwhile, GOP lawmakers representing some of the states
with the lowest life expectancy — Mississippi (71.9 years), West
Virginia (72.8 years) and Kentucky (73.5 years) — declined to comment or
did not respond to repeated questions about whether the issue
represents a public health problem.
“It’s a hard sell with senators who live in some of the lowest longevity states. And it breaks my heart,” Warren said.
Alabama Sen.
Tommy Tuberville — one of the few Republicans whose office said he was
“deeply concerned about this trend” — linked America’s decline to drug
overdoses, suicides and alcoholism.
“The
facts show clearly that this is being driven largely by an increase in
deaths of despair, with fentanyl overdoses being the leading cause of
death for Americans 18 to 45,” Tuberville spokesman Steven Stafford said
in a statement, pointing to legislation to improve mental health
funding and secure the Southern border.
In comparison, Sanders has repeatedly called for sweeping reforms, insisting in an interview that “a failed health-care system is tied into a corrupt political system dominated by enormously powerful corporate interests.”
Even
Democrats in neighboring states offered significantly different
diagnoses. In the eyes of Rhode Island Sen. Sheldon Whitehouse (D), the
No. 1 cause of America’s life expectancy problem is clear: broken
payment incentives for doctors and hospitals.
“Americans are just much less physically and spiritually healthy than they have been in a long time,” said Murphy, who has proposed a bill to create a White House office of social connection.
Ten
senators singled out the burden of chronic disease, echoing The Post’s
own review, which found that among people younger than 65, chronic illness erases more than twice as many years of life as all the overdoses, homicides, suicides and car accidents combined.
In
New York, officials are trying to put a framework around those often
abstract challenges. Vasan urged the City Council in November to support HealthyNYC, his agency’s initiative backed by Mayor Eric Adams (D) that seeks to avert about 7,300 premature deaths by 2030.
“We
want New Yorkers to experience more birthdays, weddings and
graduations, more holidays and holy days, more life lived,” Vasan told
the lawmakers, citing targets for reducing chronic diseases, cancers and
other drivers of premature death. Council members are considering
legislation to ensure that future leaders stick to the commitments — a
suddenly urgent need with Adams embroiled in a fundraising scandal.
“We
wanted this to be something that outlives us, that actually helps
people,” said Lynn Schulman, chair of the City Council’s health
committee.
Vasan
and Schulman said HealthyNYC can be a template for other cities — the
latest effort in New York’s long history of trying to tackle life
expectancy. Under former mayor Mike Bloomberg, the city raised cigarette
taxes, banned smoking in workplaces and attempted to limit sale of
large sugary drinks. When Bloomberg left office in 2013, New Yorkers’
projected life expectancy was 81.1 years — more than two years longer
than the national average — compared with 77.9 years when he took office
in 2001.
“If you want
to live longer, you could move to New York — or just vote for me,”
Bloomberg said in a speech to Democratic voters during his short-lived
2020 presidential campaign. (Public health experts have cautioned that
it may take decades to fully understand the link between Bloomberg’s
initiatives and longer life expectancy.)
But
Bloomberg’s efforts provoked backlash from food-makers, industry groups
and some elected officials. Even as New York took steps a decade ago to
limit salt and soda consumption, GOP lawmakers in other states crafted
legislation to prevent their own local leaders from taking similar
steps.
The
Bloomberg legacy “is not a torch anyone has really wanted to carry,”
said Yglesias, warning that the former mayor’s public heath agenda would
be politically difficult to replicate elsewhere. “Conservatives really
don’t like it. … I think it’s fallen out of style on the left as well.”
Sanders,
who has spent years pushing for sweeping changes to America’s health
system and economy, said Washington’s work to boost life expectancy
could begin with a simple framing device.
“The
administration, the Congress should have upon their wall, a chart which
says … ‘What’s our life expectancy now [and] how do we get up to the
rest of the world?’” Sanders said. He pointed to Norway’s life
expectancy of more than 83 years. “That should be our goal.”
An
“integrated care center” brings doctors, physiotherapists, social
workers and pharmacists under one roof. It won’t solve Britain’s
underlying social care crisis — but it could help.