Montana Experiment Brings NHS-Style Health Care to USA; Saves State Millions, Patients Delighted
by James 321
by
Former Montana Gov. Brian Schweitzer has pledged his support for single-payer health care in the past, but his recent efforts to bring zero-cost sharing primary and preventive care to Montana government employees and retirees may be doing something that most progressives would only dream could happen in America: bringing NHS-style, socialized medicine to Montana.
This is a big deal and -- while currently limited to state employees and retirees -- could be laying the groundwork for America's most socially-just health care system. NPR has the details:
A year ago, Montana opened the nation's first clinic for free primary healthcare services to its state government employees. The Helena, Mont., clinic was pitched as a way to improve overall employee health, but the idea has faced its fair share of political opposition.
A year later, the state says the clinic is already saving money.
Pamela Weitz, a 61-year-old state library technician, was skeptical about the place at first.
"I thought it was just the goofiest idea, but you know, it's really good," she says. In the last year, she's been there for checkups, blood tests and flu shots. She doesn't have to go; she still has her normal health insurance provided by the state. But at the clinic, she has no co-pays, no deductibles. It's free.
That's the case for the Helena area's 11,000 state workers and their dependents. With an appointment, patients wait just a couple minutes to see a doctor. Visitation is more than 75 percent higher than initial estimates.
Even so, division manager Russ Hill says it's actually costing the state $1,500,000 less for healthcare than before the clinic opened.
"Because there's no markup, our cost per visit is lower than in a private fee-for-service environment," Hill says.
Physicians are paid by the hour, not by the number of procedures they prescribe like many in the private sector. The state is able to buy supplies at lower prices.
Bottom line: a patient's visit to the employee health clinic costs the state about half what it would cost if that patient went to a private doctor. And because it's free to patients, hundreds of people have come in who had not seen a
doctor for at least two years.
This story shows what a little political leadership can do. Too bad there's not more of it around.
-SPC
by
Former Montana Gov. Brian Schweitzer has pledged his support for single-payer health care in the past, but his recent efforts to bring zero-cost sharing primary and preventive care to Montana government employees and retirees may be doing something that most progressives would only dream could happen in America: bringing NHS-style, socialized medicine to Montana.
This is a big deal and -- while currently limited to state employees and retirees -- could be laying the groundwork for America's most socially-just health care system. NPR has the details:
A year ago, Montana opened the nation's first clinic for free primary healthcare services to its state government employees. The Helena, Mont., clinic was pitched as a way to improve overall employee health, but the idea has faced its fair share of political opposition.Even so, division manager Russ Hill says it's actually costing the state $1,500,000 less for healthcare than before the clinic opened.A year later, the state says the clinic is already saving money.Pamela Weitz, a 61-year-old state library technician, was skeptical about the place at first."I thought it was just the goofiest idea, but you know, it's really good," she says. In the last year, she's been there for checkups, blood tests and flu shots. She doesn't have to go; she still has her normal health insurance provided by the state. But at the clinic, she has no co-pays, no deductibles. It's free.That's the case for the Helena area's 11,000 state workers and their dependents. With an appointment, patients wait just a couple minutes to see a doctor. Visitation is more than 75 percent higher than initial estimates.
"Because there's no markup, our cost per visit is lower than in a private fee-for-service environment," Hill says.Physicians are paid by the hour, not by the number of procedures they prescribe like many in the private sector. The state is able to buy supplies at lower prices.Bottom line: a patient's visit to the employee health clinic costs the state about half what it would cost if that patient went to a private doctor. And because it's free to patients, hundreds of people have come in who had not seen adoctor for at least two years.
-SPCThis story shows what a little political leadership can do. Too bad there's not more of it around.
The Trans-Pacific Partnership — Is It Bad for Your Health?
June 10, 2015DOI: 10.1056/NEJMp1506158
International trade deals once focused primarily on tariffs. As a result, they had little direct effect on health, and health experts could reasonably leave their details to trade professionals. Not so today. Modern trade pacts have implications for a wide range of health policy issues, from medicine prices to tobacco regulation, not only in the developing world but also in the United States.
The Trans-Pacific Partnership Agreement (TPP) is a case in point. A massive trade deal now reportedly on the verge of completion, the TPP has nearly 30 chapters. A draft chapter on intellectual property (IP) alone runs 77 single-spaced pages.
The full health implications of the TPP are hard to judge, not only because its provisions are complex but also because the draft text is a closely held secret. Even members of the U.S. Congress can see it only if they agree not to talk publicly about it and if they leave their pens and phones (and, until recently, their expert staffers) at the door. But several key chapters have recently been leaked and reveal that the TPP could have a substantial impact on health.
Groups including Médecins sans Frontières and Oxfam warn, for example, that the agreement could threaten the lives of millions of people in developing countries. Their concerns stem primarily from the leaked IP chapter and the effect that patents have on the prices of medicines. In the context of human immunodeficiency virus, for example, patents increase the annual cost of antiretroviral therapy from around $100 per person to $10,000 per person.
The TPP could impose obligations on developing countries that go far beyond any existing trade agreement. Indeed, some proposals in the leaked IP chapter seem directly targeted against innovative measures that developing countries have used to maximize the use of low-cost generic medicines.
For example, India allows patents on new drugs but not on new uses of old drugs or new forms of known drugs that do not increase therapeutic efficacy. These provisions have paved the way for generic versions of lifesaving drugs such as the cancer treatment imatinib mesylate (Gleevec) in that country.1 But such limits on patent eligibility could be outlawed by the TPP. Reports suggest that there may be some kind of phase-in period for developing-country members, but only for some parts of the agreement. And at best, a phase-in period would merely postpone some of the TPP's effects for a few years.2
India is not a party to the TPP negotiations, which have been conducted by 12 Pacific Rim countries: Australia, Brunei, Canada, Chile, Japan, Malaysia, Mexico, New Zealand, Peru, Singapore, the United States, and Vietnam. Why, then, would India's laws — sometimes word for word — be targeted in the TPP negotiations? For one thing, other developing countries have started to follow India's lead. For another, the TPP is a platform agreement designed for other countries to join, and it will establish a new baseline for future international negotiations. The risk regarding access to medicines in developing countries is real.
Though it is less widely recognized, the TPP could also have a direct effect on health in developed countries. For example, the leaked IP chapter contemplates major extensions of “data exclusivity” provisions. These laws prevent drug regulatory agencies like the Food and Drug Administration from registering a generic version of a drug for a certain number of years — and as a result can substantially affect the prices of medicines.
In recognition of this fact, President Barack Obama's fiscal year 2016 budget proposes rolling back the data-exclusivity period for biologic drugs in the United States to 7 years from 12 years, yielding a projected savings of more than $4 billion over the next decade.3 In the TPP negotiations, however, the United States is proposing a 12-year term of exclusivity. Such a requirement would lock the United States into a policy that many observers, including, apparently, the President himself, believe inflates the cost of medicines unjustifiably. Even if the number of years required by the TPP is negotiated downward, the lock-in effect remains a concern, because trade agreements can be extremely difficult to amend.
The cost of medicines is no small concern in the United States today: spending on prescription drugs in the United States jumped 13% in 2014 alone. The recent experience with new hepatitis C treatments shows that even lifesaving cures may be rationed in the United States — whether implicitly or explicitly — if we fail to contain drug costs and promote more efficient innovation. The TPP, however, could make moves toward more rational drug pricing in the United States difficult and even imperil existing provisions that help to contain costs for government programs.
A 2011 “annex” to the TPP, apparently proposed by the United States, would have mandated that all countries use “competitive market-derived prices” or benchmarks that “appropriately recognize the value” of the drug in question when establishing drug prices. A just-leaked December 2014 draft omits these provisions but still contemplates substantial procedural obligations for governments and makes clear that these rules apply to the Centers for Medicare and Medicaid Services (CMS). The text is difficult to decipher and still in flux. But consumer groups argue that the annex could create opportunities for interference in the decisions of CMS and render health programs in all TPP countries more vulnerable to drug-company influence and more difficult to reform.4
In March 2015, a third bombshell dropped: a draft chapter on “investor-state dispute settlement” (ISDS). It would empower foreign companies to sue member countries for hundreds of millions of dollars in damages in a wide range of cases in which they argue that their expected future profits have been undermined. These challenges would be heard by “arbiters” — typically private lawyers, many of whom cycle in and out of industry — with no prospect of independent review by a national court. Such provisions have been included in trade agreements before. But the scale of the TPP would substantially increase the number of companies that could bring such challenges. Firms have already used provisions like these to challenge an astonishing range of laws, from minimum-wage laws in Egypt, to tobacco regulations in Uruguay and Australia, to core aspects of patent law as they apply to medicines in Canada. The ISDS provisions alone could interfere with domestic health policy for decades to come. Under their auspices, policies covering a wide range of issues, from food and tobacco labeling, to patent law, to drug-pricing rules, to environmental protection could be challenged in participating countries — including, of course, the United States.
The course that the TPP takes is not yet set in stone. Negotiations continue, and the Obama administration could work toward an agreement that excludes provisions such as ISDS and the health care “annex” or that incorporates robust safeguards to protect health. Congress has an important role, too. As of early June, it was in the midst of a fierce legislative battle over whether the TPP and deals like it should be “fast-tracked.” If Congress takes this route, its ability to influence the treaty will be much diminished: fast tracking allows passage of a trade treaty with only a simple majority vote in Congress and also denies Congress any opportunity to make changes to the agreement's text.
Much hangs in the balance in the coming weeks and months. If the TPP includes robust ISDS provisions and the expansive provisions proposed in the IP chapter and the health care annex, the United States could be signing away its authority to regulate critical aspects of health policy for years to come.
Health care gobbling up resources for other government services
Here’s a chart for California that complements one I’ve posted for Massachusetts. It tells the same story; health care is drawing an increasing proportion of resources, leaving less for other government functions.
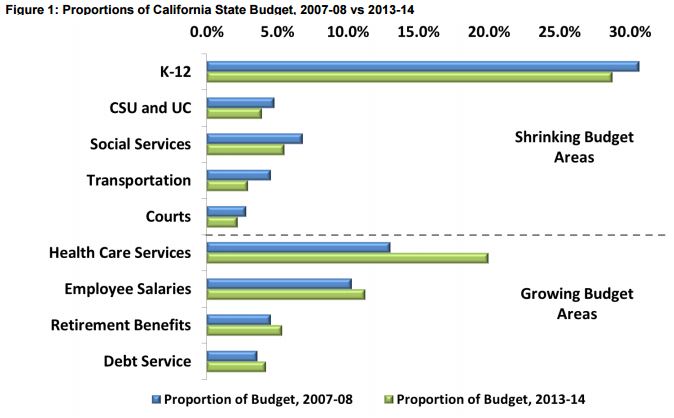
The chart is from a California Common Sense report.
The growing proportion of the California state budget devoted to health care is even higher than the “Health Care Services” bars of this chart suggest. A great deal of “Retirement Benefits” growth is due to health care too.
Annual state contributions to retirement benefits – pensions and retiree health care – have increased $1.5 billion, or 24.8% []. In particular, annual retiree health care payments have increased $682 billion, and thus account for nearly half of the retirement cost growth. Furthermore, among annual retirement costs to the state, health care for retired employees and their beneficiaries grew the most – 61.2%. By comparison, annual pension contributions increased $790 million, or 16.4%.
We should not overlook the likely possibility that many of the services losing budget, in relative terms, also probably contribute to health, and may do so more efficiently than some direct health care spending: education, social services, and transportation.
California official: Supreme Court risks 'horrible moral precedent' on Obamacare
CHAD TERHUNE
CHAD TERHUNE
The head of California's Obamacare exchange says the U.S. Supreme Court risks setting a "horrible moral precedent" if it strikes down health-law subsidies across much of the country.
Peter Lee, executive director of Covered California and a former Obama administration official, said a court ruling against the Affordable Care Act "signals that subsidies don't matter."
"I think it would set a horrible moral precedent if the Supreme Court was to find that we can leave Americans without that financial leg up," Lee said in an interview. "I think it’s a fundamental flaw to not understand how every American needs a leg up."
A court ruling against the Obama administration in the King vs. Burwell case would have no immediate effect on Covered California and its 1.2 million consumers receiving subsidies because it's a state-run marketplace.
That means justices could eliminate health insurance subsidies in as many as 37 states that use the federal HealthCare.gov marketplace. A decision is expected later this month.
Michael Cannon, director of health policy studies at the Cato Institute, said Lee and other health-law allies have it all wrong in their legal analysis.
"It would be immoral for the Supreme Court to let the president get away with breaking the law," Cannon said. "The president’s allies are panicking because they are afraid people will learn how much the Affordable Care Act costs."
Lee said he is concerned that an adverse court ruling could trigger revisions to the health law that would affect all state exchanges and possibly reduce the amount of federal assistance available to consumers.
People can qualify for subsidies if they make less than four times the federal poverty level, which is about $47,000 annually for a single adult and $97,000 for a family of four.
"Any revisions to the Affordable Care Act that back away from giving folks the financial help they need is backing away from giving people the care they need," Lee said.
The legal challenge brought by conservative activists argues that a strict reading of the health law makes subsidies available only in states such as California that established their own exchange.
That means justices could eliminate health insurance subsidies in as many as 37 states that use the federal HealthCare.gov marketplace. A decision is expected later this month.
Michael Cannon, director of health policy studies at the Cato Institute, said Lee and other health-law allies have it all wrong in their legal analysis.
"It would be immoral for the Supreme Court to let the president get away with breaking the law," Cannon said. "The president’s allies are panicking because they are afraid people will learn how much the Affordable Care Act costs."
Lee said he is concerned that an adverse court ruling could trigger revisions to the health law that would affect all state exchanges and possibly reduce the amount of federal assistance available to consumers.
People can qualify for subsidies if they make less than four times the federal poverty level, which is about $47,000 annually for a single adult and $97,000 for a family of four.
"Any revisions to the Affordable Care Act that back away from giving folks the financial help they need is backing away from giving people the care they need," Lee said.
400 Million Lack Basic Health Services, Report Finds
By RICK GLADSTONE
JUNE 12, 2015
At least 400 million people lack access to essential health services, the World Health Organization and World Banksaid Friday in a new report that they described as a “wake-up call” about the challenges to achieving universal health coverage.
The report also said that at least 6 percent of people in 37 low-and-middle-income countries are living in poverty because of the money they must spend on health. That finding alone suggested that the poorest could be left further behind by rising global health costs.
“The world’s most disadvantaged people are missing out on even the most basic services,” Dr. Marie-Paule Kieny, assistant director-general for health systems and innovation at the W.H.O., said in a statement announcing the 98-page report, which was released online and at a news conference at United Nationsheadquarters in New York.
Dr. Timothy G. Evans, senior director of health, nutrition and population at the World Bank Group, said the report’s findings illustrated the vulnerability of the world’s poorest people to health expenses.
“This report is a wake-up call,” he said. “It shows that we’re a long way from achieving universal health coverage.”
While the findings in the report, “Tracking Universal Health Coverage,” were not necessarily surprising, its creators said they had nonetheless established benchmarks for measuring both health coverage and financial protection from the cost.
They said the findings would help assess whether United Nations member states were advancing the widely asserted aspiration of universal health coverage.
“As the saying goes, ‘what gets measured, gets done,’ ” said Michael Myers, managing director at The Rockefeller Foundation, which helped support the work in creating the report.
The findings could also help measure progress in the proposed Sustainable Development Goals, part of a broader agenda undertaken at the United Nations. The 17 goals include ending poverty and hunger and ensuring healthy lives and well-being for all ages.
More Mainers With Insurmountable Medical Bills Turning to 'Crowdfunding' for Help
By PATTY WIGHT
FALMOUTH, Maine - People use crowdfunding for all sorts of things - to make movies, create new products...and to cover health expenses. A number of Maine families are turning to sites such as GoFundMe to raise money to pay looming medical bills and related expenses.
Even some of those who have insurance coverage find they still need extra financial support. But there are some drawbacks to the strategy.
Shortly after Henry Morgan's first birthday in April, the typically happy baby became fussy. He lost his appetite. It took a few trips to the doctor before he was diagnosed with inoperable neuroblastoma - it's a cancerous mass in his abdomen.
His mom, Meghan Morgan, says he's been in the hospital for nearly a month. "It looks like this is definitely going to be the next six months or so, is going to be the more intensive treatment stuff. So we're going to be staying in the hospital."
Morgan hopes they can return to their home in Falmouth periodically. But she's unable to work at her dog-walking business, and she has to pay a $5,000 deductible on her son's insurance plan. The lost income and medical bills prompted Morgan's friends and family to set up a fundraising campaign on the website GoFundMe.
Morgan says she was initially opposed to the idea. "First of all, it never would have occurred to me to ask someone for help. I'm a single mom, I'm very independent. It's just me and Henry, and that's great."
But Morgan has been floored by the response. The goal was to raise $20,000. So far, it's raised more than twice as much. "I mean, it's so overwhelming. So many strangers. People from all across the country. And my favorite is when they leave wonderful little notes in the comments, like 'Thinking of you from Maryland.' "
According to a written statement from GoFundMe, medical campaigns have always been one of its most popular categories, raising nearly $230 million since the website launched in 2010. Recent high-profile crowdfunding campaigns in New England have used the site.
By PATTY WIGHT
FALMOUTH, Maine - People use crowdfunding for all sorts of things - to make movies, create new products...and to cover health expenses. A number of Maine families are turning to sites such as GoFundMe to raise money to pay looming medical bills and related expenses.
Even some of those who have insurance coverage find they still need extra financial support. But there are some drawbacks to the strategy.
Shortly after Henry Morgan's first birthday in April, the typically happy baby became fussy. He lost his appetite. It took a few trips to the doctor before he was diagnosed with inoperable neuroblastoma - it's a cancerous mass in his abdomen.
His mom, Meghan Morgan, says he's been in the hospital for nearly a month. "It looks like this is definitely going to be the next six months or so, is going to be the more intensive treatment stuff. So we're going to be staying in the hospital."
Morgan hopes they can return to their home in Falmouth periodically. But she's unable to work at her dog-walking business, and she has to pay a $5,000 deductible on her son's insurance plan. The lost income and medical bills prompted Morgan's friends and family to set up a fundraising campaign on the website GoFundMe.
Morgan says she was initially opposed to the idea. "First of all, it never would have occurred to me to ask someone for help. I'm a single mom, I'm very independent. It's just me and Henry, and that's great."
But Morgan has been floored by the response. The goal was to raise $20,000. So far, it's raised more than twice as much. "I mean, it's so overwhelming. So many strangers. People from all across the country. And my favorite is when they leave wonderful little notes in the comments, like 'Thinking of you from Maryland.' "
According to a written statement from GoFundMe, medical campaigns have always been one of its most popular categories, raising nearly $230 million since the website launched in 2010. Recent high-profile crowdfunding campaigns in New England have used the site.
No comments:
Post a Comment