Patient-centered capitalism: redefining ethics in the medical industry
by Brian Jackson - STAT - September 24, 2019
Corporate misbehavior in the health-care
sector is widespread: irresponsible opiate marketing, misrepresentation
of research data, price gouging, and on and on. Some see it as
capitalism run amok.
In one sense, this isn’t surprising. As the Business Roundtable acknowledged in a recent statement,
American companies have too long prioritized shareholders and profits
over the interests of employees, customers, and communities. Health-care
companies are businesses, so why shouldn’t we expect them to act the
same way?
Why? Because health care isn’t just another consumer product. It is
more than that. The Hippocratic ideals of putting patients first are
ingrained in our culture and reflected in the regulation of medical
licenses and malpractice law. But although Hippocratic ideals have long
been the basis of expectations for medical professionals, they haven’t
yet been formally applied to health care companies. This is a major
shortcoming in an era when the actions of large health systems,
pharmaceutical companies, device companies, and insurance companies can
have even greater effects on patients than the actions of individual
clinicians.
advertisement
All of which is why I, a physician working in the clinical laboratory
industry, am excited about the growing interest in stakeholder
capitalism that the Business Roundtable laid out: for a business to be
sustainable over the long term, it must explicitly address the interests
of all major stakeholders. Owners (shareholders) are an
important stakeholder group, but so are customers, employees, and the
community in which the business operates.
Of all industry sectors, I am convinced that health care has the
most to gain from this model. Health care may also have the clearest
path to stakeholder capitalism due to some of its distinctive
characteristics.
First, the health-care industry includes groups that share a common
ethical culture and language. These include physicians, nurses,
scientists, and other professionals, all of whom are schooled in medical
ethics during training. It also includes mission-driven hospitals and
health systems, including many with religious affiliations.
Second, health care will find it easier than many other industries to
find the right balance among its various groups. The doctrine of
shareholder supremacy has a certain elegance in that it simplifies the
decision about which group comes first — shareholders. Medical ethics
and patient-centered capitalism offer an equally elegant solution:
patients come first and all others, including shareholders, come second.
Third, health care has a mature and well-defined set of ethical
principles against which to measure corporate behavior. The ethical
codes of the American Medical Association and the American Nurses Association are well-known examples, though they are worded specifically for individual practitioners. Another example is the Belmont Report,
commissioned by the U.S. government in 1978, which laid out rules for
conducting research on human subjects. All of these codes are based on
three core principles: respect for persons, beneficence, and justice.
Respect for persons includes autonomy and informed consent. If
medical device manufacturers followed this principle, they would have to
disclose to patients how likely they will be to actually benefit from a
particular hip replacement or pacemaker or cardiac stent. They would
also have to disclose whether there might be a competing device with a
higher success rate and a lower complication rate.
Beneficence includes the Hippocratic maxim of “Do no harm.” If
oxycodone and fentanyl manufacturers had followed this principle, they
would not have downplayed the abuse potential of these drugs in their
marketing messages to doctors.
Justice involves fairness for all patients. Health insurers following
this principle would need to ensure equitable coverage across all ages,
genders, disease categories — including mental health — and among
vulnerable populations.
Fourth, health care guided by patient-centered capitalism offers a
rich set of structural opportunities for accountability to all
stakeholders. Large health systems and group-purchasing organizations,
for example, have enormous market power over suppliers of medical
products. This power is currently leveraged mainly to obtain lower
prices, but it can just as easily be used to preferentially choose
suppliers whose marketing meets scientific standards of objectivity, who
contribute all clinical data to public registries, and who meet other
defined standards.
Likewise, medical professionals such as physicians and nurses have
enormous potential influence on health care companies. They can openly —
and ideally collectively — declare their expectations regarding the
companies they work for and whose products they use, and then back up
these statements with their career choices and medical product choices.
There is an obvious accountability role for regulatory agencies in
patient-centered capitalism such as the Food and Drug Administration and
the Centers for Medicare and Medicaid Services, but distributed mutual
accountability will be more robust than one-directional regulation
alone.
Changing corporate culture across an industry as huge as health care
will take time. But the barriers can be overcome. And the Business
Roundtable just took away one of them — the business doctrine of
shareholder supremacy — or at least signaled a willingness to do so.
The public expects and deserves ethical actions not just from
individual health care workers but also from the organizations and
companies in this sector. It’s time we make this happen.
Patient-centered capitalism can point the way. https://www.statnews.com/2019/09/24/patient-centered-capitalism-redefine-ethics-health-care/
Employer Health Insurance Is Increasingly Unaffordable, Study Finds
A
relentless rise in premiums and deductibles is putting insurance out of
reach for many workers, especially those with low incomes.
by Reed Abelson - NYT - September 26, 2019
Jessie McCormick had to quit her job to afford health care.
Ms.
McCormick, 27, who has a heart condition, had an opportunity to move
from part time to full time in her job at a small nonprofit in
Washington. Working full time would qualify her for the firm’s health
plan.
But she calculated that her out-of-pocket costs would be at
least $1,200 per month, about double the money she had left after
paying her rent and utilities.
Instead, she quit her job last
summer so her income would be low enough to enroll in Medicaid, which
will cover all her medical expenses. “I’m trying to do some side jobs,”
she said.
Employers remain the main source of health insurance in
the United States, covering about 153 million people. But premiums and
deductibles are pushing employer-based coverage increasingly out of
reach, according to a new analysis released Wednesday by the Kaiser Family Foundation, which conducts a survey of employers every year.
The
average premium paid by the employer and the employee for a family plan
now tops $20,000 a year, with the worker contributing about $6,000,
according to the survey. More than a quarter of all covered workers and
nearly half of those working for small businesses face an annual
deductible of $2,000 or more.
The new data on
employer coverage come as the Democratic presidential candidates debate
sweeping reforms to diminish the role of private insurance in the
American health system, including expanding the federal Medicare program
to everyone or giving people the option to enroll in a government-run
plan.
Many of the arguments for both systems center on expanding
health insurance to more of the estimated 27 million people who lack it.
But millions of people who already have coverage are deeply
dissatisfied with the current system as well.
“For some reason, we
like to focus on coverage when the issue for workers, people and the
public generally is cost,” said Drew Altman, the chief executive of the
foundation. About 2,000 small and large businesses responded in detail
to the survey.
Small employers in particular, and their workers, are struggling.
“Health
insurance in the United States is incredibly prohibitive for small
businesses,” said Shalin Madan, the founder of a small investment
advisory firm in Florida. He is not required to provide health insurance
to his workers, because his business is too small and he outsources
much of the work.
A policy for his own family, he said, runs about
$2,000 a month ($24,000 per year), with a $13,000 deductible. “I’m out
$37,000 before I see a return on investment, if you will,” Mr. Madan
said.
A recent Wall Street Journal/NBC News poll found that a
majority of registered voters, 56 percent, are opposed to the idea of a
government-run system like Medicare-for-all that would replace private
insurance. But Mr. Madan said the current system results in a schism
between those who have good employer coverage and those who do not.
“I had phenomenal health insurance being employed,” said Mr. Madan of his time working for a larger corporation.
One
of Senator Elizabeth Warren’s applause lines on the Democratic
presidential campaign trail is that no one likes their insurance
company. But employer coverage “isn’t monolithic,” said Mr. Altman.
While
some people, usually higher-paid professionals or union members, enjoy
generous coverage from their job, people making $25,000 or less — about
36 million Americans — are the most likely to be priced out of coverage,
he said.
People who work at companies where a large share of the
employees are low-wage workers pay an average of $7,000 annually for a
family plan, according to the survey, about $1,000 more than those
working at companies made up of better-paid workers.
Only
one in three of these workers is enrolled in an employer’s plan, about
half the rate at better-paying companies. “This is a group that really
deserves a lot more attention,” Mr. Altman said.
While some
low-wage workers may qualify for Medicaid in states that expanded it
under the Affordable Care Act, those with private insurance who are not
eligible for government help are having a more difficult time affording
care, said Dr. Benjamin Sommers, a health economist at the Harvard T.H.
Chan School of Public Health.
“The arc of the A.C.A. really tried, and largely succeeded, in leaving the employer market as is,” he said.
For
many businesses, it’s a Sophie’s choice between raising an employee’s
share of premiums or increasing the size of the deductible.
“I
try to keep the benefits pretty much the same,” said Joel Sturm, chief
operating officer of the New York College of Podiatric Medicine. The
majority of workers are in a plan that comes with a deductible of $1,000
for an individual and asks them to pay about 10 percent of their
medical bills. “It doesn’t kill them if they go,” Mr. Sturm said.
But
the employees must pay a hefty share of the overall premiums, about
$950 a month for a couple. Some employees have quit as a result of
having so much taken out of their paycheck and still having to cover
some out-of-pocket costs, Mr. Sturm said. “They’d rather be unemployed
than have very little take-home pay,” he said, adding that Medicaid can
seem like a more attractive option.
Image A
tag on Ms. McCormick’s backpack. Koda, her medical alert dog, can smell
when Ms. McCormick’s blood pressure drops, usually signaling an
imminent fainting spell.CreditSamuel Corum for The New York Times
Many
businesses have opted to increase deductibles instead of premiums. “A
lot of employers with lower-paid employees want to offer a low-cost
option that is typically a high-deductible plan,” said Chris Bartnik, a
senior vice president at Lockton Companies who advises businesses on
their coverage.
But some of his clients who once
embraced high deductibles have changed their minds, worried their
workers can’t afford to go to the doctor.
Some large employers are
adjusting the premiums and deductibles based on an employee’s income.
JPMorgan Chase pays 80 percent of the premiums for workers making under
$60,000, and the company lowered the annual deductible by $750 to $2,000
or less, depending on the plan they choose.
(JPMorgan Chase is also part of the trio of big corporations behind Haven, a new venture trying to reinvent employer-based coverage.)
H.A.
Cover & Son Lumber, in Thayer, Mo., has decided to pay the bulk of
premiums for workers, but the plans come with a deductible of $2,500 for
an individual and $5,000 for a family. The company is paying about
$16,000 a month to cover the 11 people enrolled in the plan.
The
deductible “is higher than we wanted to go,” said Marion Cowen, who
oversees benefits for the business, but the cost for more comprehensive
coverage was prohibitive. “We don’t know what we’re going to do if it
goes up much more,” she said.
She is intrigued by the idea of
being allowed to buy into a government plan, like Medicaid or Medicare,
that is being floated by some of the candidates. “We would consider it,
yes, we would,” she said, if the option saved money and provided
employees with high-quality coverage.
The
Wall Street Journal/NBC News poll found that about two-thirds of voters
supported the idea of allowing people to buy into Medicare. “Some states
are looking at a public option,” said David Chase, who leads the
national outreach efforts for Small Business Majority, an advocacy group
that supported the Affordable Care Act. He said the group is talking to
various states about allowing small businesses the option of buying
into a government program.
“There are a lot of hypothetical
proposals out there,” said Neil Trautwein, vice president of health care
policy at the National Retail Federation, who said his members are
increasingly concerned about rising health care costs. Companies are not
as keen on offering less generous plans, he said, but would be open to
other alternatives.
At Bagel Grove in Utica, N.Y., most of the 20 employees are now covered by Medicaid, said Anne Wadsworth, one of the owners. She
took advantage of the tax credits available to small businesses that
helped pay for the cost of coverage under the Affordable Care Act, but
the credits ran out. While she still covers 45 percent of the premiums,
all but one of her employees, herself included, have found better plans
on their own.
“I was all on board for Obamacare,” she said, but
it proved not to be “a long-term solution. It doesn’t lower the costs
for people.”
Ms. Wadsworth is wary of the sweeping plans now
proposed by the Democratic presidential candidates, which she worries
will become a political football, like the Affordable Care Act, and fail
to address the underlying issues.
“I just think health care costs need to go down,” she said. https://www.nytimes.com/2019/09/25/health/employer-health-insurance-cost.html?
Why the Private Health Insurance Industry Faces an Existential Crisis
A former health insurance executive says the moment the insurance industry fears most has arrived.
by Wendell Potter - Common Dreams - September 24, 2019
I have told a lot of stories about my time near the top of the health
insurance industry. This is not one I’ve ever shared, until now.
Shortly before I left Cigna, I was at a meeting of the company’s
senior executives. This was as then-presidential candidate Barack Obama
was gaining traction in national polls and filmmakers like Michael Moore
were documenting how broken our health insurance system had become. Our
CEO at the time, Edward Hanway, had just been asked a simple question
by the company’s top attorney: “What keeps you up at night?”
He responded without hesitation. “Disintermediation.”
I had never heard the term and had to look it up. The definition: cutting out the middleman.
This is a watershed moment for Medicare for All and America’s health insurance companies.
What scared us most at the health insurance companies was our place
on the priority list for patients. We know people want to see their
doctor, visit their preferred pharmacy or attend any hospital in an
emergency. This makes doctors, dentists, pharmacists and nurses
essential to the delivery of health care. They’re the faces of it.
Behind the scenes are companies that make drugs and machines important
to treatment, along with people who conduct research and implement
health policies.
Our health insurance companies, in contrast, are not essential. They
don’t treat anyone. They don’t prevent anyone from becoming sick. They
don’t take you to the hospital or make sure you take your pills. They
don’t fund or discover medical innovations. They’re simply middlemen we
don’t need. And in the industry, we always dreaded the day American
businesses and patients would wake up to that reality.
That day has come.
SCROLL TO CONTINUE WITH CONTENT
A majority of America’s small businesses now support Medicare for All. So do a majority of Americans who receive health insurance
through their employer. In my 20 years working inside the industry and
the 11 years I’ve been watching from the outside, I have never seen such
high support among the people who get their coverage through their
employers for switching to a publicly financed, privately delivered
health care system.
This is a watershed moment for Medicare for All and America’s health
insurance companies. Fifty-eight percent of nonelderly Americans receive health insurance
through their employer. Now most of them—and their employers who pay
handsomely to provide insurance—have decided they’d rather work with the
government (through an improved and expanded Medicare program) than
continue a relationship with private insurers. That is a stunning rebuke
of the private sector, though not one that has been unforeseen, as
health insurers charged an average of $6,715 per insured employee last year—and $20,000 for a family plan—according to the Kaiser Family Foundation.
There are two things to note about how the insurance industry has
responded to this development: they’ve simultaneously tried to prevent
change and prepared for the unraveling of the employer-based system.
The evidence for both is the “Coverage@Work”
PR and lobbying campaign America’s Health Insurance Plans launched last
year. Even though the percentage of nonelderly Americans enrolled in
employer-sponsored plans has declined from 67 percent to 58 percent over
the past decade, despite the Affordable Care Act mandating insurance be
given to all full-time employees, companies like the one I used to work
for continue to make a lot of money on these kinds of plans. The
industry wants to keep employers in the game as long as possible, though
they’ve known for more than a decade that the employer-sponsored health
insurance system is collapsing.
They’ve also known that we have an aging population, which is why big
insurers have placed such a big bet on Medicare Advantage, the private
alternative to traditional Medicare. Insurers devote a substantial
portion of their sales and marketing budgets to lure Medicare-eligible
Americans into Medicare Advantage plans. The bet has been paying off:
more than half of some of the big insurers’ revenue (including
UnitedHealthcare, the biggest insurer) is now coming from federal and
state governments. A growing percentage is coming from their Medicare
Advantage business and also from the Medicare supplement plans they
sell, as well as from their Medicare Part D pharmacy plans and the
Medicaid programs they operate under lucrative contracts with most
states.
As he was elaborating on disintermediation, Cigna’s CEO said his fear
was that someday American employers and their workers would begin to
question the “value proposition” of private health insurers. That’s
business-speak for something not being worth what you’re paying for it.
That someday has arrived for America’s job creators. They are waking up
to realize the middleman is not necessary. It’s time for our policymakers to wake up, too.
Rebecca Grimm tried to be a smart shopper when her second pregnancy ended in a miscarriage last year.
Grimm,
who has a high-deductible health plan, first tried a $10 pill to clear
the fetal tissue. When that didn’t work, she checked her insurance
company website to compare the cost of a surgical procedure at several
local medical centers.
All were around $900, she recalled. Grimm went to a center a few miles from her house. The procedure took 20 minutes.
The Grimms got a bill for $5,948.69.
“We thought something had to be wrong,” said Grimm, who is 29 and
lives in a small house in the northern suburbs of Indianapolis. “Having a
miscarriage was hard. Having to deal with medical bills for months
afterwards was like salt in the wound.… It made no sense at all.”
High-deductible
health plans, which are fast becoming the dominant form of coverage for
U.S. workers, were supposed to empower patients. Backers said the plans
would create engaged shoppers who would check prices and compare
providers, forcing hospitals, doctors and drugmakers to control costs.
Deductibles have more than tripled over the last decade
for people who get insurance through their jobs, but the promised
consumer revolution never materialized. Instead, Americans have been
left shopping in the dark and increasingly struggling with medical bills
they can’t afford, a Times examination of job-based health insurance
shows.
“This idea that we were going to give patients ‘skin in the
game’ and a few shopping tools and this was going to address the broad
problems in our healthcare system was poorly conceived,” said Lynn
Quincy, former healthcare advocate at Consumer Reports now at Altarum, a nonprofit research and consulting firm.
“It’s clear now that the idea definitely hasn’t borne fruit,” Quincy
continued. “It hasn’t made people feel more confident seeking care. It
hasn’t led to better value. And it’s had terrible consequences on
patients’ ability to afford care.”
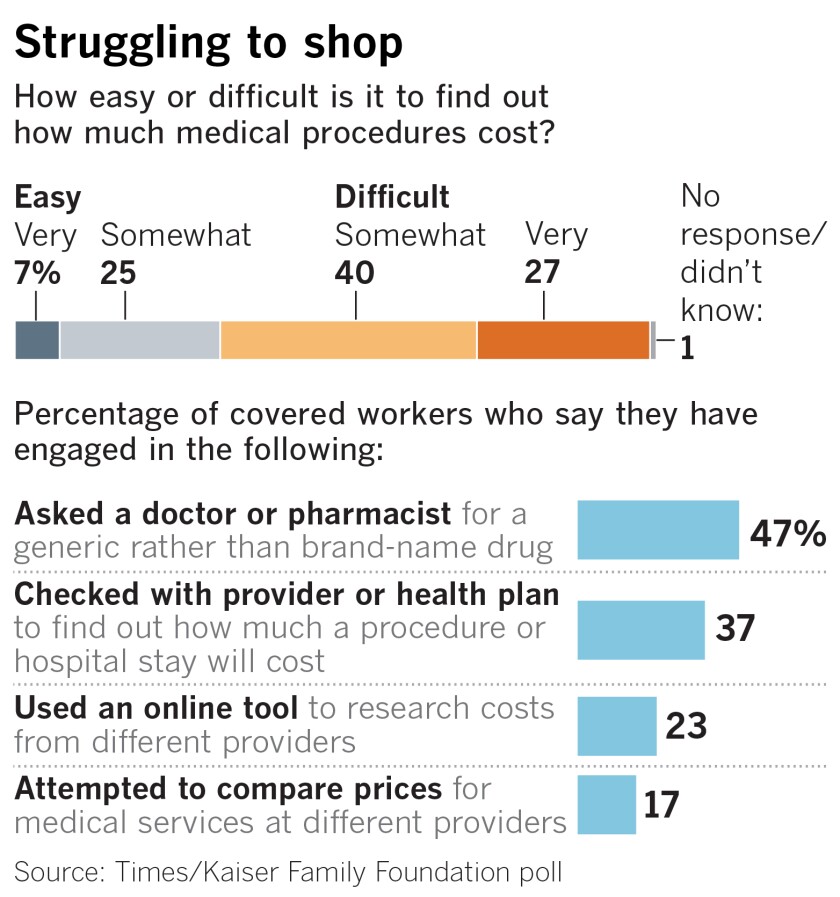
Although Americans are willing to seek out lower-priced generic
medications, few are comfortable shopping for medical care, studies and
surveys show. Patients like Grimm who do try are often frustrated by
incomplete or inaccurate information from insurers, hospitals and other
medical providers.
Just 1 in 6 covered workers even tried to shop for the best price for a medical service in the previous year, according to a nationwide poll
conducted for this project by The Times and the nonprofit Kaiser Family
Foundation. Two-thirds of workers with job-based coverage said finding
the cost of a medical treatment or procedure was somewhat or very
difficult.
Meantime, prices for medical care and prescription
drugs haven’t moderated, as advocates of high-deductible insurance
predicted. Instead, they have soared.
The average price of a knee replacement, for example, shot up nearly
80% between 2003 and 2017, increasing at more than double the rate of
overall inflation, a Kaiser Family Foundation analysis of commercial insurance data found.
These
price hikes are crushing insured Americans: 1 in 6 workers with
job-based benefits in the Times/Kaiser Family Foundation poll reported
that they had to make a “difficult sacrifice” in the past year to pay for healthcare, such as cutting back on food and other essentials.
“We overestimated the ability of consumers to be good stewards of
their healthcare dollars in a system that is very unfriendly to
consumers, and underestimated the support they would need from us,” said
Dr. Marcus Thygeson, a former Blue Shield of California executive who
worked on early efforts to develop so-called consumer-directed health
plans.
Early champions of high-deductible health insurance —
including benefit consultants, conservative health-policy advocates and
Republican politicians such as former House Speaker Newt Gingrich —
promised something very different when they sold employers on shifting
more costs onto workers in the early 2000s.
Rebecca Grimm plays with her 2-year-old daughter, Amelia, and husband, Mark, at their home in Westfield, Ind.
(Leah Klafczynski / For The Times)
“When consumers apply pressure on an industry, whether it’s retailing
or banking, cars or computers, it invariably produces a surge of
innovation that increases productivity, reduces prices, improves quality
and expands choices,” Harvard Business School professor Regina
Herzlinger wrote in an influential 2002 essay. Herzlinger became a leading proponent of having patients put more “skin in the game.”
By some measures, healthcare markets appeared ripe for an intervention.
Then and now, prices for the same medical service can vary dramatically from one hospital or doctor’s office to another.
In
Philadelphia, for example, the price of a colonoscopy ranges from less
than $1,000 at some hospitals to nearly $4,000 at the most expensive,
researchers at the Health Care Pricing Project found by analyzing commercial health insurance data from around the country.
Similarly,
the lowest-priced hospitals in Houston billed as little as $15,000 for a
knee replacement, while the costliest charged more than $35,000.
That kind of price variation — which has little relationship to
quality, according to a growing number of studies — spawned online tools
that were supposed to help patients find the most economical place to
get care.
“There was this notion that if people could figure out
where to buy the cheapest Kleenex, they could pick doctors and
hospitals, too,” said Dr. Arnie Milstein, medical director of the
California-based Pacific Business Group on Health, an organization of large companies including Boeing, Safeway, Walmart and Wells Fargo.
Finding medical care is more complex than choosing facial tissue, however. And few workers ended up using these tools.
In one study
of nearly 150,000 people covered by two large national employers, only
about one in 10 who could shop for price information did, even if they
had a high-deductible plan. And use of the tool was not associated with
lower healthcare spending.
In the Times/Kaiser Family Foundation
survey, only about a quarter of workers with job-based coverage reported
using an online cost tool.
Americans show little inclination to
find the best deal even for a basic medical service like an MRI scan,
which can be as much as five times more expensive in one facility than
in another, another recent study found.
Researchers
analyzing commercial insurance data from tens of millions of Americans
reported only 14% of patients went to the lowest-cost MRI within a
30-minute drive of their house. Patients on average passed six
lower-priced MRI facilities on their way from home to the place where
they had the imaging, the study found.
Many Americans don’t want to have to shop for healthcare, preferring to let their physicians guide their care.
“We
pretty much go where we’re comfortable. We’re not looking for the
cheapest doctor,” said Jim Morrissey, 39, a food service manager who
lives near Harrisburg, Pa. “I’m loyal to the doctors I trust.”
Americans’ lack of enthusiasm for medical shopping also reflects how little information is available about prices.
The wildly inaccurate estimate that Grimm got for her procedure in Indiana is hardly unique.
When researchers in 2011 and 2012 called a sample of 122 hospitals
across the country to get a price for a hip replacement, a common and
usually straightforward elective surgery, only 19 were able to provide a
complete estimate, including the hospital and physician costs.
Even
when the researchers called a physician’s office separately to get
doctors’ fees, they could get a full estimate less than half the time.
Four years later, when a second group of researchers repeated the exercise with the same hospitals, the results were worse: Only eight gave a complete estimate.
Information on the quality of medical services, which patients would need to be informed shoppers, is even harder to come by.
Hospitals
that can provide a single price for something like a hip replacement
typically “bundle” all the services required for the procedure,
including the surgeons’ fees, the anesthesia, the use of any medications
and the cost of using hospital facilities such as the operating and
recovery rooms.
But that’s not the way most medical care in the
U.S. is billed. Rather than a single price, hospitals, doctors and other
medical providers rely on approximately 10,000 individual billing codes
to charge for services. A consumer who wanted to shop would have to
price each service separately.
When Grimm finally succeeded in
getting an itemized bill from the surgical center, she and her husband
were floored by the 23 individual charges, including: $65.23 for
Lidocaine, an anesthetic; $133.28 for two injections of Ondansetron, a
drug to prevent nausea and vomiting; $413 for oxygen; $132.80 for a
liter of sterile water.
There were two charges for the surgery itself of $2,380 and $9,782. Grimm’s brief stay in the recovery room cost $720.
“How in the world were we supposed to know how to shop for all that?” she said.
Herzlinger,
the Harvard Business School professor, said in a recent interview that
the consumer revolution she envisioned didn’t occur because hospitals
and doctors resisted efforts to make healthcare pricing more
transparent.
“There are a lot of people who don’t want this
information revealed,” she said, adding she never believed
consumer-directed healthcare required high deductibles. “I personally
think deductibles are too high,” she said.
Shopping becomes even more unrealistic for a person with an emergency — chest pain, for example, or an automobile accident.
Nor
would a patient have either the ability or much incentive to compare
costs for a complex disease like cancer that may require months of
chemotherapy, radiation and other expensive and often-unpredictable
medical services, the price of which would likely exceed even the
highest deductibles.
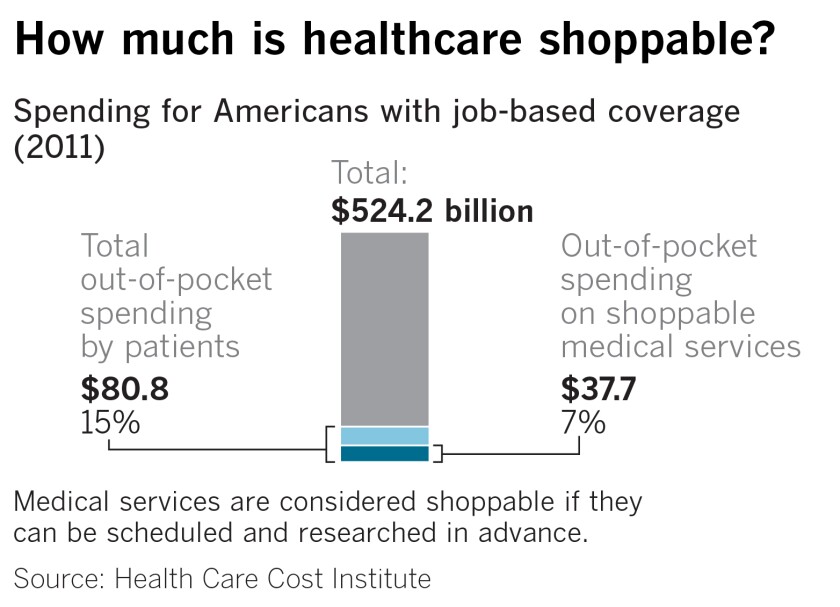
By one estimate
by the Health Care Cost Institute, just 7% of total healthcare spending
for Americans with job-based coverage was on medical services that
could be considered “shoppable” because the service required an
out-of-pocket payment and the procedure could be researched in advance.
“The
fact is very little medical care is shoppable,” said David Newman, the
institute’s former director, noting that medical care is not like other
services that Americans typically buy.
“We become good shoppers
when we are repeat shoppers,” he said. “If you buy a new car every three
years, you can become an informed shopper. There is no way to become an
informed shopper for your appendix. You only get your appendix out
once.”
Julie Hernandez, a 61-year-old graphic designer in Oregon,
discovered the limits of medical shopping the hard way when she went to a
dermatologist earlier this year to get a small cancerous growth removed
from her nose.
Sensitive to costs, in part because she had a
high-deductible plan, Hernandez tried to get estimates from several
medical offices in her area around Medford. She selected what seemed to
be the lowest-cost option, even though she was told the procedure might
cost $3,000 to $8,000.
Midway through the surgery, after the
doctor had removed several layers of skin from Hernandez’s nostril to
take off the cancerous tissue, the doctor asked Hernandez as she lay on
the operating table whether she wanted to have the wound closed with
skin from her cheek or from another part of her nose.
“I had a
gaping hole the size of a dime in my nose,” she said. “At that point,
money didn’t come into play. I went with the option the doctor said was
best.”
Hernandez later got a bill for $5,568.
As for the
Grimms, they ultimately got a discount for Rebecca’s procedure after she
spent months filling out forms and negotiating with the surgery center.
They ended up paying $2,300.
But as she prepared to have a second
baby this summer, the couple didn’t even try to shop for the best
price, though they knew they’d have to pay thousands of dollars for the
delivery. https://www.latimes.com/politics/story/2019-09-25/shopping-medical-care-lots-of-luck?
Nurses in Four States StrikPush for Better Patient Care
Registered nurses with National Nurses United say current nurse-to-patient ratios do not allow for the best possible care.
by Aimee Ortiz - NYT - September 20, 2019
Thousands
of nurses across the country went on strike Friday morning, pushing for
better patient care by demanding improved work conditions and higher
pay.
About 6,500 National Nurses United members at 12 Tenet
Healthcare hospitals in California, Arizona and Florida organized a
24-hour strike, which began at 7 a.m., to protest current
nurse-to-patient ratios that they contend are burning out employees and
making it difficult to provide the best possible care.
In
Chicago, more than 2,000 nurses walked off the job after contract
negotiations between National Nurses United and the University of
Chicago Medical Center broke down on Wednesday night.
“We’re here
to advocate for our patients,” said Yajaira Roman, an intensive care
unit nurse who works for Tenet Healthcare’s Palmetto General Hospital in
Hialeah, Fla., and a member of the union’s bargaining committee. “We’re
pretty much urging the hospital to invest in the nurses and take steps
to strengthen our recruitment and retention of experienced nurses at the
hospital.”
“It’s very difficult to give a patient optimal care if our patient ratio is so high,” Ms. Roman said.
Research
shows that with “every patient over four assigned to one nurse in a
medical surgical unit, there’s an increase in mortality of 7 percent per
patient,” she said, noting her hospital currently allows for eight
patients to one nurse.
A strong contract between the union and
the hospital, Ms. Roman said, helps ensure that patients receive the
best possible care. National Nurses United members in all four states
have been working either without a contract or under an expired one. The
strikes in Arizona and Florida are the first by registered nurses in
those states, the union said.
Fawn Slade, a registered nurse at St. Joseph’s in Tucson and a union member, echoed the concerns about patient ratios.
“If we did not feel that this was necessary to get a strong contract, we would not be out here doing this,” Ms. Slade said.
In
Arizona alone, 37,000 people with active registered nurse licenses
don’t work as nurses, Ms. Slade said. “We are hopeful that this strong
contract will bring those nurses back to the bedside.”
In a
statement on Friday, Tenet Healthcare said the company’s top priority
“is providing our patients with excellent care, as always.”
“Our
hospitals are fully operational with dedicated and experienced nurses,
caregivers and supporting staff delivering high-quality, compassionate
care throughout today’s one-day strike,” a Tenet spokeswoman said.
The
hospital system did not give specific nurse-to-patient ratios, but the
spokeswoman said, “Our hospitals are staffed appropriately.”
“The
safety of our patients is paramount and staffing decisions are made to
support this based on acuity and individualized needs of each patient,”
she said.
The University of Chicago Medical Center also brought in
temporary nurses to cover its gaps in staffing during the one-day
strike, contracting them for five days — a move union members saw as
retaliation for the demonstration.
“They chose to lock us out for
these five days,” said Talisa Hardin, a registered nurse at the
center’s burn unit. She said that the hospital deactivated the badges of
striking nurses and removed their parking privileges, and that meant
that nurses would lose five days of pay, Ms. Hardin said.
Debi
Albert, the hospital’s chief nursing officer, said the temporary
nurses, who came in from across the country, would come in only for a
five-day contract.
“The competition for those relief nurses was
quite high,” Ms. Albert said. The staffing agency used to hire the
temporary nurses, she said, indicated to the hospital that “if we wanted
to safely staff the hospital for one day, we had to commit to those
nurses for five days, or they would not travel.”
In addition to
hiring the temporary nurses, the University of Chicago Medical Center
moved several patients out of the neonatal intensive care unit, the
pediatric intensive care unit and the intensive care unit. The
hospital’s emergency room is currently on diversion, meaning ambulances
must find somewhere else to go, even if it is the closest one.
“It’s
heartbreaking” that they’re moving patients, Ms. Hardin said. “You work
in a place and you think that there’s values and that what you do
matters, and they do things like take your patients away.”
The
nurses at the University of Chicago Medical Center face unsafe working
conditions daily, according to Ms. Hardin. She said that units often
borrow supplies, equipment and even staff from one another just to make
ends meet.
“It’s kind of a robbing-Peter-to-pay-Paul situation,” Ms. Hardin said.
The University of Chicago Medical Center, through a spokeswoman,
rejected the notion that the hospital was inadequately staffed.
“As
in any hospital, we often see unpredictable and sudden increases in
demand for care within our inpatient units,” she said. But she noted
that the hospital has a group of nurses who can shift between units
depending on need.
Speaking in a video
message before the strike, Sharon O’Keefe, president of the University
of Chicago Medical Center, said Thursday, “We’re disheartened that we
had to get to this point.”
The hospital “worked long and hard
negotiating with the help of a federal mediator and had hoped union
leadership would meet us halfway,” she said. “We now have to focus our
efforts on safely operating our hospitals and caring for the patients
who depend on us.”
Friday’s nurses’ strikes add to a growing list
of union actions that have taken place across the nation recently,
including the continuing United Auto Workers strike and the Los Angeles teachers’ strike earlier this year. https://www.nytimes.com/2019/09/20/us/nurse-strike.html?
On
Monday, the United Nations High-Level Meeting on Universal Health
Coverage took place in New York, convening leaders from all countries to
reinforce political commitment toward health care for all by 2030.
Dozens
of countries have universal coverage models in place, and many low- and
middle-income countries are making great strides; ironically, the
meeting’s host country, the United States, is a strong outlier.
A large percentage of the United States’ gross domestic product is spent on health care, yet life expectancy and health outcomes compare poorly with other high-income countries spending much less. Although fewer Americans live in poverty today, an increased number live without health insurance. A need for emergency care may put these families in financial distress or, worse, on the streets.
On
Monday, the United Nations High-Level Meeting on Universal Health
Coverage took place in New York, convening leaders from all countries to
reinforce political commitment toward health care for all by 2030.
Dozens
of countries have universal coverage models in place, and many low- and
middle-income countries are making great strides; ironically, the
meeting’s host country, the United States, is a strong outlier.
A large percentage of the United States’ gross domestic product is spent on health care, yet life expectancy and health outcomes compare poorly with other high-income countries spending much less. Although fewer Americans live in poverty today, an increased number live without health insurance. A need for emergency care may put these families in financial distress or, worse, on the streets.
If
not these, then what are strong enough incentives to protect the
Affordable Care Act as a steppingstone to move toward health care for
all?
‘Value’ of Care Was a Big Goal. How Did It Work Out?
by Austin Frakt - NYT - September 23. 2019
A period of Medicare innovation has resulted in more ‘singles than home runs.’
“It
doesn’t mean that the vast majority of the care Medicare purchases is
linked to actual value,” said Sherry Glied, a health economist, and dean
and professor at the Wagner School of Public Service at N.Y.U. “We
don’t even know what we mean by value. How do you pay for something when
you don’t know what it is?”
Different programs have different notions of “value.” Medicare’s Hospital Readmissions Reduction Program,
established in 2010, penalizes hospitals that have high rates of
readmissions for certain illnesses. Although hospitals can lose only up
to 3 percent of payment, 100 percent of their payment is considered
“tied to value.”
The key is whether programs like this improve
health care quality or reduce health care spending. The Hospital
Readmissions Reduction Program has been extensively examined, with
studies drawing different conclusions. Initial analyses of the program suggest it is responsible for reducing hospital readmissions, saving Medicare billions of dollars a year.
But some later studies found that these reports of success were overstated, among other concerns. Some studies found that reduced hospital readmissions were associated with increased risk of death, though not all studies
agree on this point, and experts disagree on the value of the program.
What is clear is that the program has had a smaller impact on hospital
readmissions than originally thought — perhaps reducing them by as
little as one-third of a percentage point.
Another Medicare value-based payment program is considerably more broad. The Hospital Value-Based Purchasing Program
was introduced in 2011 and rewards or penalizes hospitals based on
mortality; infection rates; patient experience and safety; cost; and
other measures of quality — 20 in all. Typical bonuses or penalties are a fraction of 1 percent of a hospital’s total Medicare payments.
A study published in
Health Services Research compared about 2,800 hospitals in the program
with about 300 exempt from it. The study found no effect from financial
incentives of the program on quality of care or patient satisfaction.
But the study included data only up to nine months after the program’s
start, and it may take hospitals longer to make measurable changes.
Another study, published in BMJ, looked at outcomestwo
and a half years after the start of the Hospital Value-Based Purchasing
Program. It found no differences in changes in mortality rates between
hospitals in the program versus those exempt from it. And another study,
published in Health Affairs, found no evidence that the program improved patient satisfaction up to three years after implementation.
Jose
Figueroa, a physician at Brigham and Women’s Hospital in Boston, and an
assistant professor of medicine at Harvard Medical School, was an
author of both of these longer studies. “So far, there’s no evidence the
program has improved quality or patient satisfaction,” he said. He
ticked off some possible reasons: “The financial incentives are too weak
to drive any meaningful changes across hospitals. The program’s design,
with numerous measures across different domains, makes it hard for
hospitals to understand what to focus on.”
Medicare has achieved
greater success with programs that have raised the stakes — ones that
have put hospitals and health care organizations at greater risk of
financial loss or have offered prospects for larger financial gain.
One
popular approach, called “bundled payments,” pays health providers one
amount for all of the care for a certain condition within a certain
period — like 90 days for hip replacement care. There is evidence that some of these programs can save money without reductions in quality, although design details matter.
“Bundled
payments are a straightforward way to make hospitals consider all the
costs they are responsible for,” said Adam Sacarny, assistant professor
with Columbia’s Mailman School of Public Health. “The evidence suggests
they encourage hospitals to treat patients more efficiently, although
the cost savings are at least partly offset by extra payments to
hospitals to reward them for saving money in the first place.”
Another
approach — accountable care organizations — also takes many forms. What
they have in common is they offer health care organizations the chance
to earn bonuses for accepting some financial risk, provided they meet a
set of quality targets. Many studies of accountable care organizations (A.C.O.s) have found they reduce spending with no quality degradation.
“There
is strong evidence that, on average, Medicare A.C.O.s save a modest
amount of money,” said Alice Chen, assistant professor at the University
of Southern California Sol Price School of Public Policy.
Although accountable care organizations have saved a few percent of Medicare spending, the amount varies
by program design. “We’ve found that A.C.O.s that are physician groups
as opposed to big hospital systems have produced more savings,” said
Michael McWilliams, a professor at Harvard Medical School and a general
internist with Brigham and Women’s Hospital. “That’s because physician
groups don’t erode their own revenue when they keep their patients away
from hospitals.”
So over all, is Medicare moving toward higher
value? “There has been some progress, but even the most generous read of
the evidence is very far below the projections made by fans of value-based payment before the A.C.A.,” Ms. Glied said.
Robert
Berenson, a fellow at the Urban Institute, agreed: “Value payment
overemphasizes performance measurement, but even so, it’s been
disappointing. We simply lack good metrics that can’t be gamed or evaded
by most targeted providers.”
But some are more optimistic. “The
successes are more like singles than home runs,” said Michael Chernew, a
health economist with Harvard Medical School. “Despite the modest
results, I think some approaches, like A.C.O.s, are a foundation for
future improvements.”
Paying for health care value is a popular slogan, but Medicare is still figuring out how to do it. https://www.nytimes.com/2019/09/23/upshot/medicare-health-value-costs.html?
Pelosi Offers Medicare Negotiation Plan to Curb Drug Prices
by Associated Press - September 19, 2019
WASHINGTON — House Speaker Nancy Pelosi, trying to seize
the agenda on a top consumer issue, announced an ambitious prescription
drug plan Thursday that would allow Medicare to negotiate prices for
seniors and younger people.
The proposal would direct Medicare to
bargain over as many as 250, but no fewer than 25, of the costliest
drugs. Insulin is on the list. Drugmakers that refuse to negotiate could
face steep penalties. Companies that raise prices beyond inflation
would have to pay rebates to Medicare.
The plan would limit copays
for seniors covered by Medicare's "Part D" prescription drug program to
$2,000. Medicare-negotiated prices would be available to other buyers,
such as employer health plans.
It's shaping up as a high-stakes
gamble for all sides in Washington. Polls show that high drug prices
have Americans worried, and regardless of party affiliation, they want
Congress to act. As a candidate, President Donald Trump called for
Medicare negotiations but later seemed to drop the idea.
Pelosi, D-Calif., said her goal is a deal that Trump can sign onto and that could pass the GOP-controlled Senate.
"We
don't want a political issue at the polls," Pelosi said at a news
conference. "We want a solution in Congress, and we want it now."
Weighing
in on Twitter, Trump said, "Let's get it done in a bipartisan way!"
Unlike other Republicans, he refrained from criticizing Pelosi's bill
and said "it's great" to see her out with a plan. But he said he
preferred a bipartisan Senate bill being pushed by Iowa Republican Chuck
Grassley.
In the Senate, Republican John Cornyn of Texas said
Pelosi's proposal "has absolutely no chance —zero, zip, nada" of
passing. Some House Republicans quickly dismissed it as "socialism."
The
2003 law that created Medicare's prescription drug benefit barred the
program from negotiating prices, a restriction Democrats have long
opposed. Most Republicans say they believe price negotiations are best
left to private players such as insurance companies.
The
industry group Pharmaceutical Research and Manufacturers of America
said Pelosi's plan was "radical" and would usher in an era of government
price-setting that would "blow up" the current system, stifling
innovation. But health insurers called the plan "bold reform" and
hospitals said it takes "significant strides toward reducing
out-of-control drug prices." Public Citizen, a consumer group on the
political left, said the bill didn't go far enough because it left
intact drugmakers' monopoly on new medicines.
A leading House
progressive, Texas Democrat Lloyd Doggett, agreed that more is required.
"This new bill was promoted as a way to sway President Trump and a
reluctant Republican Senate," said Doggett. "I await their embrace."
While
the legislation leans left politically it also incorporates ideas from
the Trump administration and from Republican and Democratic senators — a
signal Pelosi wants a deal.
Pelosi's proposal would:
—
authorize Medicare to negotiate prices for up to 250 drugs with the
greatest total cost to society. That includes pharmacy drugs under the
Part D prescription benefit, and Part B medications dispensed in
doctors' offices, such as many cancer drugs. Medicare would negotiate
for as many drugs as possible on a list refreshed annually, but no fewer
than 25. The maximum price would be determined using a blend of
international prices, similar to a more limited proposal from the
administration. Drug companies that balk at making a deal would face
penalties that start at 65% of sales for the drug at issue, and escalate
if they hold out.
— require drugmakers to pay rebates to Medicare
if they raise prices beyond the increase in inflation. That idea
resembles the plan from Sens. Grassley and Ron Wyden, D-Ore. Their
proposal has cleared a key committee, with Trump's support. But many
Senate Republicans oppose inflation rebates, and it's unclear what
Majority Leader Mitch McConnell, R-Ky., plans to do next.
— limit
what seniors pay out of pocket for their medications to $2,000 a year.
Currently, Medicare's pharmacy benefit has no cap on copays, and the
advent of drugs costing hundreds of thousands of dollars a year has left
some seniors saddled with bills that rival a mortgage payment. An
out-of-pocket limit is part of the Grassley-Wyden bill and is backed by
the administration.
For now, criticism of the industry — from Trump and lawmakers of both parties — appears to be having an effect on prices.
The
Commerce Department's inflation index for prescription drug prices has
declined in seven of the past eight months, which is highly unusual.
That index includes lower-cost generic drugs.
For brand-name
drugs, a recent Associated Press analysis shows prices are still going
up on average, but at a slower pace. Costly brand-name drugs that
translate to steep copays are the top concern for consumers.
The
AP analysis found that in the first seven months of 2019, drugmakers
raised list prices for brand name medicines by a median, or midpoint, of
5%. That's a slowdown. Prices were going up 9% or 10% over those months
the prior four years.
Still, there were 37 price increases for every decrease in the first seven months of 2019.

 “It’s clear now that the idea definitely hasn’t borne fruit,” Quincy
continued. “It hasn’t made people feel more confident seeking care. It
hasn’t led to better value. And it’s had terrible consequences on
patients’ ability to afford care.”
“It’s clear now that the idea definitely hasn’t borne fruit,” Quincy
continued. “It hasn’t made people feel more confident seeking care. It
hasn’t led to better value. And it’s had terrible consequences on
patients’ ability to afford care.”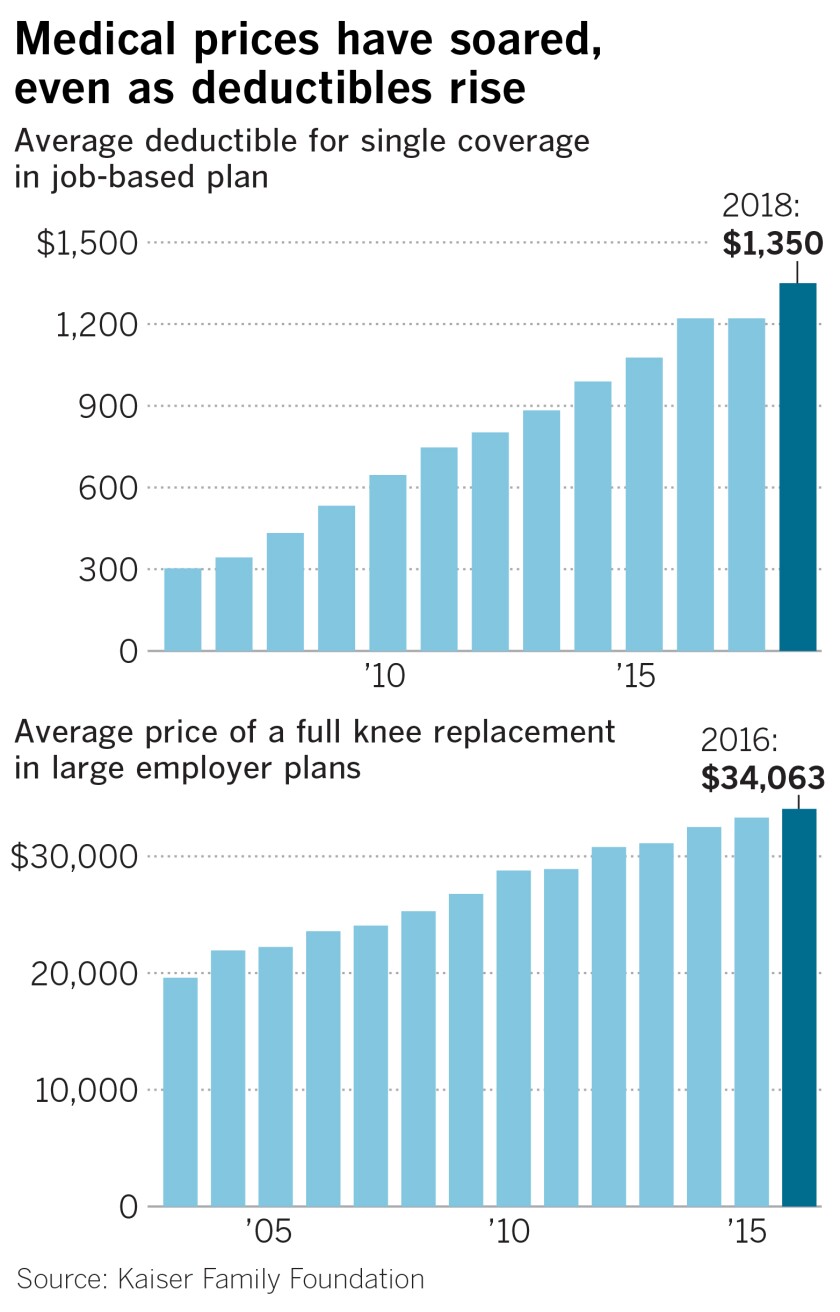

No comments:
Post a Comment