Ex-UN chief Ban Ki-moon says US healthcare system is 'morally wrong'
Former United Nations secretary general Ban Ki-moon has denounced the United States’ healthcare system as politically and morally wrong, and urged American leaders to enact publicly-financed healthcare as a “human right”.
Ban made the comments in an exclusive interview with the Guardian in New York, as part of his work with The Elders, a group founded by Nelson Mandela to work on issues of global importance, including universal health coverage.
The US has the world’s most expensive health system, accounting for nearly one-fifth of American gross domestic product and costing more than $10,348 per American. The United Kingdom, by comparison, spends a little under 10% of GDP according to the latest available statistics, and healthcare is free at the point of delivery.
“It’s not easy to understand why such a country like the United States, the most resourceful and richest country in the world, does not introduce universal health coverage,” said Ban. “Nobody would understand why almost 30 million people are not covered by insurance.”
Failing to provide health coverage, he said, was “unethical” and “politically wrong, morally wrong”. He accused the “powerful” interests of pharmaceutical companies, hospitals and doctors that “inhibit the American government” of having prevented the US from moving towards universal healthcare.
“This is for the people. Leaders are elected because they vowed that they would work for the people,” said Ban. “They are abandoning people because they are poor, then these poor people cannot find a proper medical support.”
Despite astronomical spending on health, millions in the US live entirely outside the health system, uninsured and unable to go to the doctor without incurring hundreds or thousands in debt. Since President Trump was elected, an additional 4 million people have lost health coverage, according to a recent survey by the Commonwealth Fund.
“It seems with Trump just undoing Obamacare, people were not happy first of all,” said Ban, about health reforms enacted to weaken elements of the Affordable Care Act, former President Barack Obama’s signature healthcare law. “Ironically, it might have motivated people to think other ways, and influence their senators, and their Congressman to think the other way.”
Ban revealed he had his own run-ins with the American healthcare system. While he was Secretary General between January 2007 and December 2016, the UN provided him with American health insurance. About three years ago, he set out to pick up a prescription at a pharmacy, but forgot his insurance card. A worker at the pharmacy told him that without insurance, his prescription would cost $200. If he came back with his insurance card, it would be $20.
“It was totally unfair,” said Ban. “People like myself can afford [this]. But poor people cannot afford it. They do not have any support.”
“While swearing in as Secretary General, I pledged I would make this world better for all,” he said. “Nobody would imagine that there should be so many people – 30 million people – who would be left behind” in the US.
Health coverage has become a major issue ahead of the Congressional midterm elections in November, which are widely seen as a referendum on Trump’s America.
Progressive Democrats have called for Congress to enact “Medicare-for-all”, a proposal to expand the public health program which covers all Americans older than 65. Establishment Democrats have argued for expansions of Obamacare.
As well, four conservative states are attempting to expand Medicaid, the public health insurance program for the poor and disabled, through a ballot referendum.
Trump and Republicans have worked to make health coverage more exclusive. The Trump administration has allowed states to add work requirements to public health programs for the poor and disabled, and Republicans ended a requirement for Americans to buy private health insurance when they cut taxes.
Ban blamed the “sectoral interests” of pharmaceutical companies, hospitals and doctors, “which inhibit the American government” for hindering moves towards a universal health coverage plan.
“Here, the political interest groups are so, so powerful,” Ban said. “Even president, Congress, Senators and Representatives of the House, they cannot do much so they are easily influenced by these special interest groups.”
Ban said he hopes states, including California and New York, will pass universal health coverage and spark a national call for public financing of health.
“It will be either California or New York who will introduce this system,” said Ban. “Then I think there will be many more states who will try to follow suit. I think that’s an encouraging phenomenon we see.”
These Are the Economies With the Most (and Least) Efficient Health Care
by Lee J. Miller and Wei Lu - Bloomberg News - September, 2018
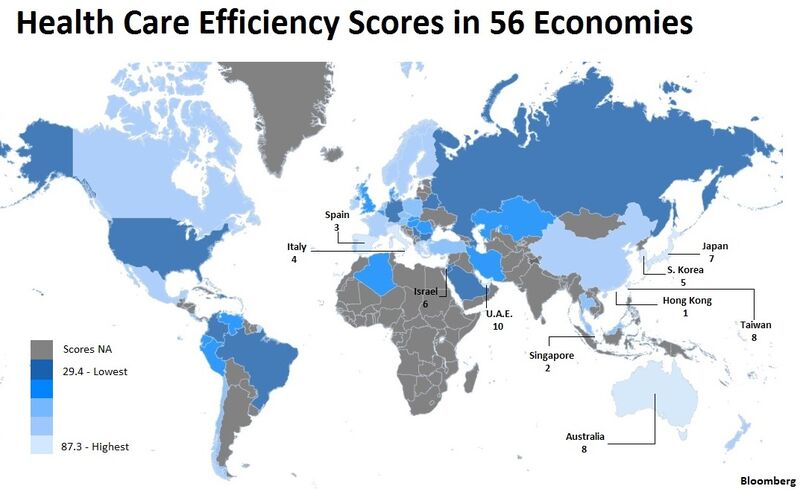
Want medical care without quickly draining your fortune? Try Singapore or Hong Kong as your healthy havens.
The U.S. will cost you the most for treatment, both in absolute terms and relative to average incomes, while life expectancy of Americans -- about 79 years -- was exceeded by more than 25 countries and territories, according to an annual Bloomberg analysis in almost 200 economies.
A health-efficiency index was then created to rank those with average lifespans of at least 70 years, GDP per-capita exceeding $5,000 and a minimum population of 5 million.
Americans aren’t getting their medical money’s worth, according to each of the categories.
The U.S. had the second-highest per-capita spending on health care at $9,536. Switzerland’s average based on gross domestic product was $9,818. But that $282 supplement helped deliver an extra 4.2 years of life -- with the average Swiss lifespan of almost 83.
READ MORE: U.S. Health system ranked among the least efficient in the world, before and during first year of Obamacare HERE, and HERE and HERE.
Compared to residents of the Czech Republic -- which had an average life expectancy almost at parity with the U.S. -- Americans spent more than double on health care relative to GDP, 16.8 percent versus 7.3 percent. Health spending is the U.S. is estimated to increase to 18 percent of GDP in the U.S., according to estimates from the Altarum Institute.
The latest reading of the Bloomberg index reflects the second full year of "Obamacare," the short name for the U.S. Affordable Care Act, which expanded access to health insurance and provided payment subsidies starting on Jan. 1, 2014. The latest health-efficiency gauge used 2015 data, as that’s the most-recent for most economies from the World Health Organization.
That lag time also puts the spotlight on the U.K., which fell out of Europe’s top 10 in the health ranking based on 2015 data. The nation voted in favor of Brexit the following year, with costs and efficiency of the National Health Service a key issue for British voters.
Spain’s health system efficiency ranked third behind Hong Kong and Singapore, followed by that of Italy, which moved up two spots from a year earlier. Italy ranked as the world’s healthiest country in a separate Bloomberg gauge.
Thailand moved up 14 places to No. 27, the biggest annual improvement, as per-capita spending declined 40 percent to only $219, while life expectancy advanced to 75.1 years. Medical tourism industry is among Thailand’s fastest-growing industries.
Chile, highest-ranked from Latin America last year, tumbled 23 positions, out of the top 10 to 31st, well behind Mexico and Costa Rica. The Chilean government spent 28 basis points more on health expenditure relative to annual GDP, while longevity of its citizens fell more than two years.
Israel and the U.A.E. ranked highest among Middle East economies, with both remaining in the top 10 from last year’s survey.
Costa Rica, Ireland, Lebanon and New Zealand were added to the final index this year, having reached the population threshold -- all now ranking among the top 25.
Rankings can change substantially year-over-year because of such things as recession, currency fluctuations and volatile spending patterns relative to the slow pace of improvement in life expectancy.
Check out the full index here:
Bloomberg Health Care Efficiency
Sources: World Bank, World Health Organization, UN Population Division, International Monetary Fund, Hong Kong Department of Health, Taiwan Ministry of Health and Welfare
Notes: Total health expenditure generally includes preventive and curative health services, family planning, nutrition activities and emergency aid; Relative cost is measured by total health expenditure as a percentage of GDP and absolute cost is the simple per capita total health expenditure in nominal dollar terms; Data as of 2015 for all economies except for Hong Kong and Taiwan in which case 2014 data was used
Maine court to hear arguments in fight over implementing Medicaid expansion
by Marina Villeneueve - AP & Portland Press Herald - September 20, 2018
A Maine court is preparing to hear the latest arguments in the state’s failure to enact voter-approved Medicaid expansion.
Expansion has been held up for months because of Republican Gov. Paul LePage’s opposition over funding issues and the resulting legal battles. A judge charged with addressing looming constitutional issues affecting Medicaid expansion has scheduled hearings for Sept. 27-28 in Portland.
Last fall, nearly three of five Maine voters supported expanding Medicaid to 70,000 to 80,000 adults with incomes up to 138 percent of the federal poverty level.
Maine’s top court recently upheld a lower court order requiring the LePage administration to file paperwork needed to start rolling out Medicaid expansion. The state submitted what’s known as a state plan amendment, but the governor urged federal regulators to reject it.
Maine’s top court left consideration of constitutional issues about Medicaid expansion to a Superior Court judge, who will begin to weigh such matters at the court hearings next week.
One issue is that the voter-approved ballot measure didn’t say how Maine would pay for its share of expansion.
Pro-Medicaid expansion groups, such as Maine Equal Justice Partners, argue that Maine, like other states, can simply rely on state general funds. Charlie Dingman, a lawyer representing the group, said he expects courts will address what should happen now that the July 2 deadline for implementing Medicaid expansion has passed and Mainers have begun applying for coverage.
“We will also be addressing the bad faith of the administration in failing to file a state plan amendment that was straightforward and designed to encourage coverage would begin,” Dingman said.
The governor’s office, meanwhile, has said the LePage administration has complied with the court order.
The governor denies estimates that expansion will save Maine tens of millions of dollars and has vowed to block Medicaid expansion until lawmakers provide funding under his terms, which include no tax increases. He vetoed a bill to fund expansion using state surplus and one-time tobacco settlement funds.
One Big Problem With Medicaid Work Requirement: People Are Unaware It Exists
by Margot Sanger-Katz - NYT - September 24, 2018
Arkansas is the first state to test it, and thousands have been kicked off the program.

The Trump administration argues that imposing work requirements for Medicaid is an incentive that can help lift people out of poverty. But a test program in Arkansas shows how hard it is merely to inform people about new incentives, let alone get them to act.
In the first month that it was possible for people to lose coverage for failing to comply, more than 4,300 people were kicked out of the program for the rest of the year. Thousands more are on track to lose health benefits in the coming months. You lose coverage if you fail to report three times, and the program, in effect for three months, is slowly phasing in more people.
Arkansas is the first state to test a work requirement, a policy that the administration has encouraged, and that several other states are hoping to copy. The demonstration project is testing whether a work requirement can help encourage more low-income people to work, volunteer or go to school and improve their financial prospects.
The early results suggest that the incentives may not work the way officials had hoped. Arkansas officials, trying to minimize coverage losses, effectively exempted two-thirds of the eligible people from having to report work hours.
Of the remaining third — about 20,000 people — 16,000 didn’t report qualifying activities to the state. Only 1,200 people, about 2 percent of those eligible for the requirement, told the state they had done enough of the required activities in August, according to state figures.
Seema Verma, the administrator of the Centers for Medicare and Medicaid Services, which approved the project, offered an enthusiastic assessment of the results so far. “I’m excited by the partnerships that Arkansas has fostered to connect Medicaid beneficiaries to work and educational opportunities,” she wrote on Twitter. (Her office declined to offer any further statements on the Arkansas experience.)
Advocates for the poor, and the state officials in charge of the program, said the low compliance numbers suggested that many eligible people probably didn’t know the program existed. State officials said they worked hard to get the word out — mailing letters, sending emails, placing phone calls, briefing medical providers, putting posts on social media sites and distributing fliers where Medicaid patients might find them.
“I was literally taking fliers to the urgent care clinic when I was taking my kids to get tested for strep,” said Amy Webb, the chief communications and community engagement officer for the Arkansas Department of Human Services. “If there’s something we are not doing to reach people, if someone will tell us how to do that, we will do it.”
But it seems that not everyone opened or read their mail. Ray Hanley, the president of the Arkansas Foundation for Medical Care, which ran a call center for the state, told my colleague Robert Pear that many people never answered their phones. The state said the open rate on emails was between 20 and 30 percent.
It’s harder to measure how many people opened paper mail, but the state noted in its recent report that it knows that thousands of people in the program either move away from their recorded address or fail to answer other mail from the state. Housing instability and moves are more common among low-income Americans.
Jessica Greene, a professor of health policy at Baruch College in New York, visited three Arkansas counties last month and interviewed 18 Medicaid beneficiaries. Twelve of them were unaware of the work requirement, according to an article she published on the website of the journal Health Affairs.
That may not be entirely surprising. “I ignore mailings and calls from my health insurer — I get them all the time,” said Eliot Fishman, a senior director of health policy at Families USA, a consumer advocacy group.
Mr. Fishman oversaw Medicaid demonstration projects in the Obama administration. He said he learned that it was challenging to use health insurance as a vehicle to shape behavior, because most people don’t read the fine print of their health benefits.
Under Mr. Fishman’s watch, Indiana tested a program to get beneficiaries to take more responsibility for their health. Medicaid patients who made small monthly payments in special accounts, got a checkup or did other activities could earn more generous benefits. Ms. Verma, then a consultant, helped the state devise that program. In an evaluation, it turned out that only a minority of eligible people understood that the accounts existed.
Joan Alker, the executive director of the Georgetown Center for Children and Families, who opposes work requirements for Medicaid, said the state could have done more to get the word out — if it had been willing to spend more.
The Obama administration spent millions on advertising and in-person help when it rolled out Obamacare’s coverage expansion in 2014. Even then, it took several years before the uninsured rate among poor Americans stopped dropping. “You cannot have an incentive strategy that is allegedly designed to change people’s behavior if people are not aware of it,” she said.
The challenge goes beyond getting the message out. The state requires those eligible for the work requirement to report their work hours every month, and only online. Arkansas has one of the lowest rates of internet penetration in the country; estimates from the Urban Institute suggest that more than a quarter of eligible families are not online.
Advocates for the poor describe the state’s website as confusing to navigate, especially for people with limited computer skills and overall literacy. (Click on the site yourself and see if you can figure out how to report work hours.) The state has tried workarounds — like offering computer terminals in county offices, and training volunteers to help people log their hours.
But evidence from a range of social programs — including Medicaid — has repeatedly demonstrated that administrative hurdles can cause eligible people to lose benefits.
As the program is expanded to more people, awareness and compliance may spread over time. But the early results could mean the end of the program before we know for sure. A lawsuit challenging the work requirement will be reviewed soon by a federal judge who already knocked down a similar work rule in Kentucky. In that case, the judge, James Boasberg, said Kentucky had been insufficiently concerned about the people who might lose coverage because of the requirement. In Kentucky, those losses were theoretical. In Arkansas, they’re already real.
https://www.nytimes.com/2018/09/24/upshot/one-big-problem-with-medicaid-work-requirement-people-are-unaware-it-exists.html?
Collins’ bills to ban pharmacy ‘gag clauses’ pass House and Senate
by Joe Lawlor - Portland Press Herald - September 26, 2018
Bills sponsored by Maine Sen. Susan Collins that ban “gag clauses” prohibiting pharmacists from telling consumers about the lowest prescription drug prices passed the House on Tuesday – after previously gaining Senate approval – and now will go to President Trump to sign.
Trump supports the measures and is expected to sign the bills, called the Patient Right to Know Drug Prices and the Know the Lowest Price Act. The bills passed the House by voice vote.
The bills were bipartisan, and in addition to Collins were authored by Democratic Sens. Claire McCaskill of Missouri and Debbie Stabenow of Michigan, and Republican Sens. John Barrasso of Wyoming and Bill Cassidy of Louisiana.
“Gag clauses” have become more common in recent years and prohibit pharmacistsfrom informing patients that paying out-of-pocket in some cases would be cheaper than using their health benefits.
“Insurance is intended to save consumers money. Gag clauses in contracts that prohibit pharmacists from telling patients about the best prescription drug prices do the opposite,” Collins said in a statement. “Who would think that using your debit card to buy your prescription drugs would be less expensive than using your insurance card? It’s counterintuitive. Americans have the right to know which payment method provides the most savings when purchasing their prescription drugs.”
The “gag clauses” are written into contracts with pharmacists by insurance companies or pharmacy benefit managers.
Pharmacy benefit managers are middlemen whom insurers pay to set up a list – called a formulary – of what drugs are covered by the health insurance plan. The formularies are designed to save money but can have unintended consequences.
Pharmacy benefit managers have existed for many years, but the changing nature of health insurance benefits – where patients are now shouldering more of the cost of prescription drugs – has brought drug pricing into the forefront.
The bills cover private insurance as well as Medicare Advantage and Medicare Part D plans.
“I am delighted that our legislation to lower the cost of prescription drugs and save consumers money received overwhelming bipartisan support in both the House and the Senate, and I look forward to it being signed into law,” Collins said in a statement.
Trump, in a tweet before the Senate passed the bills this month, said that “Americans deserve to know the lowest drug price at their pharmacy, but ‘gag clauses’ prevent your pharmacist from telling you! I support legislation that will remove gag clauses.”
by Kathy Johnson - The Chronicle Herald (Nova Scotia) - September 24, 2108
SHELBURNE, N.S. – Hundreds of Shelburne County residents took to the streets for the People over Politics march and rally to protest the current health-care crisis on Saturday, Sept. 22.
Starting at the Loyalist Plaza (Woodworkers Home Furniture) on Water Street in Shelburne, participants were joined along the route as they marched to the Community Centre on King Street, where others were waiting to show their support.
helburne Mayor Karen Mattatall, Queens-Shelburne MLA Kim Masland, Shelburne Fire Chief Darrell Locke and Roger Taylor, councillor for the Municipality of Shelburne, took the podium, all echoing the same message – the health-care system is in crisis for rural Nova Scotia and it needs to be fixed.
“The province of Nova Scotia through the NSHA (Nova Scotia Health Authority) has allowed the state of health care for all Nova Scotians, and particularly Shelburne County and other rural areas, to devolve to a deplorable state,” said Mayor Mattatall. “All parties have had a hand over the years in the demise of the system. However, it’s time to stop blaming the people in the past and fix it now. People’s lives are in jeopardy.”
Mattatall, as well as other speakers, called on the province to make health care the top of their priority list.
“Spending millions and millions of dollars on a bloated bureaucracy instead of front-line services is not addressing our needs,” she said. “We need the ER 24/7 at Roseway Hospital and we shouldn’t settle on that as a solution as it doesn’t provide everyone with a family doctor, it won’t reduce wait times, it won’t allow us access to services locally that support our demographic which is growing, and it doesn’t recognize our geography. It won’t prevent the horror stories we hear of people travelling long distances to access services that should be available right here in our own community.”
Mattatall said up until the mid-1990s, Nova Scotia had a system that worked quite well.
“The decision-making was made locally, not by a bureaucratic organization that we have no connection with. At that time, the province felt because the health-care budget was consuming 25 per cent of the province’s total budget it was unsustainable, so they hired a consultant and the consultant determined too many doctors and too many hospitals and that’s how they were going to reduce the cost,” the mayor said. “However, 20 years later it’s consuming 50 per cent of Nova Scotia’s total budget and we certainly in rural Nova Scotia are seeing about 25 per cent of the services we saw then. Rural Nova Scotians have been the victims. We’ve watched a 52-bed facility (Roseway Hospital) erode to very minimal services today.”
Queens-Shelburne MLA Kim Masland told those gathered that having this many people come out to support Roseway Hospital access and delivery sends a strong message to provincial Health and Wellness Minister Randy Delorey.
“This is a crisis and it’s a crisis our government is not admitting to,” said Masland. “After two hospital closures in Cape Breton my fear is this government is coming for us next. I’m not saying this to add to your fear. I’m saying this because I’m worried.
“In question period, I asked Randy Delorey several times to guarantee to me as long as he was minister of heath this hospital would remain an open, full-service hospital. I asked for a yes-or-no answer. He said a lot of words in reply but none of them were yes,” she said, adding she has also asked the premier the same question. “He didn’t say yes either, instead he scolded me for being so bold, that such a young politician as myself would choose so early in my career to insult a minister.”
Masland said she has heard from numerous constituents with health-care concerns.
“I listened to the fear in a young parent’s voice when they arrived at the local ER with their convulsing child to be told it’s closed and they need to call 911. I’ve listened to the concern of a cancer patient who requires access to the ER within that golden hour and fears the ER might be closed. I have shared fears of an 18-year-old boy who sat in the ER for hours desperately reaching out for mental health treatment only to leave because he couldn’t bear to have community members watching him cry,” she said. “I’ve heard the frustration of a young lady who was suffering from something as simple as a bladder infection on a Friday and was told by her physician she would need to travel to Yarmouth or Liverpool to have a urinalysis done because the lab was closed. I’ve listened to young parents who struggle to make ends meet but are forced to take time off work and travel and sit in an ER for an entire day with a sick child, all because they don’t have a family doctor at home. Senior citizens have said they are giving up because they can’t bear to travel for dialysis or sit in an ER to have a simple prescription refilled.
Masland spoke about her 84-year-old grandmother and about how she laid on an ER gurney for five days in a small examining room with no bathroom facilities and another infectious patient.
“Nurses were walking in fully gowned and masked while my grandmother lay there totally exposed. Some of her last words to me were, ‘My dear I’m too sick to be home but I’m too sick to be here,’” she said. “She died eight days later. I will never forgive the system that failed her. I will never forget the nurses and doctors who tried so hard to make things better for her, but the government was asking them to do the impossible. She deserved better and so do all of you… My message to you is do not stop fighting.”
Shelburne Fire Chief Darrell Locke said Delorey “doesn’t have a sweet clue and he doesn’t want to know.”
“He wants us to quietly go away. The minister of health wants everyone to believe the EHS system is a good substitute for the ER. EHS are a wonderful group of people who do an absolutely fabulous job. However, right now, today in Shelburne, there’s one ambulance on duty. As soon as somebody needs it, that ambulance is away from the area, so another ambulance will get shifted close to this area. That could be Exit 30 in Barrington. It could be sitting in Sable River covering Liverpool and Shelburne and right to Barrington,” he said, adding there are times that ambulances are “not readily available,” and at times when that happens there are volunteer firefighters qualified as first responders.
“In the absence of an ambulance we will come. We do the best we can with our level of training,” said the fire chief. “We do not and cannot transport patients anywhere so our level of care to you is going to be in your kitchen, your bedroom, your living room, wherever we might find you.”
Shelburne Municipal Councillor Roger Taylor said when he first started raising concerns about health care about 10 years ago, “I felt like the lone wolf, but now health care is the number-one priority of the Federation of Nova Scotia Municipalities, so it’s just not us. We can’t let the government get away with this. Let’s keep up the fight.”
A province-wide rally to bring attention to the health-care crisis is slated to be held in communities across Nova Scotia on Oct. 13. Further details will be released soon.