The View From Here: What are we talking about when we talk about Medicare for All?
Bernie Sanders' bill is more than health care reform, it's a restructuring of the national economy.
by Greg Kasich - Maine Sunday Telegram - April 14, 2109
With Bernie Sanders’ Medicare for All bill introduced in the Senate, let’s get ready for a big debate about what it really is. Most of it will take place on the Democratic presidential
campaign trail, where all the major contenders say they are for it, but
they all seem to mean something a little different. And Republicans will be having their own debate, trying to
figure out which monster under your bed is a scarier one – Medicare for
All or a Green New Deal. Before things heat up too much, it might be worth talking about
what Sanders’ version of “Medicare for All” is by starting with what it
is not. For one thing, it’s not Medicare, at least not as we know it.
Medicare is a half-century-old single-payer insurance program that
covers hospitalization and doctor visits for people who are 65 and
older, as well as younger people with disabilities. Unlike Sanders’ bill, Medicare does not cover long-term care,
and it does not cover prescription drugs, unless Medicare recipients buy
a separate, optional policy. Medicare doesn’t cover dental care or
glasses, but Sanders’ bill would. People on Medicare usually buy private insurance to supplement
their coverage unless they are low income enough to qualify for
Medicaid, the federal and state health care partnership. Sanders’ bill would wipe that out, giving everyone access to
health care without private insurance, deductibles, co-pays or any other
out-of-pocket costs. The bill does not nail down a funding source, but Sanders says
that shouldn’t be a problem. If you add up what’s spent through
government programs, employer-provided private insurance, tax
expenditures and out-of-pocket expenses, the United States already
spends more on health care than any other country in the developed world
– twice as much as Canada – and has worse results. Sanders figures we
could actually spend less on a better system. Which gets to what this version of “Medicare for All” really
is. It’s a restructuring of the economy. By reallocating who pays for
health care, Sanders would be narrowing the gap between rich and poor in
a way we have not seen since the old New Deal in the 1930s. Here’s how it might work: About half of Americans get their
health insurance through work. Right now, a CEO making $300,000 a year
and a janitor at the same company making $30,000 pay the same insurance
premium. If the employer tries to lower its costs by moving to a less
generous plan – one with higher deductibles, or fewer covered benefits –
the CEO and the janitor would have the same out-of-pocket
responsibilities, even though one’s pocket is deeper than the other’s. If both employees were covered by the new Medicare, and if it
were funded by a progressive income tax, the CEO would be paying much
more than the janitor. It would be easy to structure the tax so that
most people would be paying less for their health care. Since there are fewer rich people than not-rich ones, this should be a winning policy in a democracy. Which leads to the other thing the Medicare for All is: A theory of democratic social change. Sanders is not going to pass his bill by winning a debate in
the Senate – there will not be a debate in the Senate unless Mitch
McConnell wants one, and he doesn’t. He’s not going to lobby his buddies
in the cloakroom or the gym. Sanders doesn’t seem to like other
senators, and they don’t seem to like him. And Sanders is not going to pass his bill by getting the
hospitals, insurance companies and other interested parties to sit
around the table and hammer out a bipartisan deal that everyone can live
with. Sanders is not interested in a House bill that aims to fix some
of the flaws in Obamacare. He’s not motivated to shave a few people off
the list of the uninsured. The only way Medicare for All has a chance (at least as
envisioned by Sanders) is for its supporters to win elections, not just
the presidency but many elections all across the country. The last time any legislation approaching this magnitude became
law was 1965, the year when Lyndon Johnson signed the Voting Rights
Act, Medicaid and the original Medicare. The previous November he had
been returned to office with 63 percent of the popular vote, along with
68 Democratic senators and a 145-representative Democratic advantage in
the House. If Medicare for All is the biggest social program ever
conceived in our history, passing it would take that kind of landslide,
moved by the biggest social movement we’ve ever seen. To work in coalition with people who they don’t like very much
and focus on economic justice, millions of people would have to put
aside some issues that matter very much to them.
Over the next year, we’ll find out if that momentum exists.
It’s what we’ll we be talking about when we talk about Medicare for All.
Why Trump’s New Push to Kill Obamacare Is So Alarming
by Nicholas Bagley - NYT - March 27, 2019
Attorney General William Barr was supposed to be a voice of reason in the Trump administration. An old Washington hand, he had the stature and the backbone to protect the Justice Department from a White House that often seems to disdain the rule of law.
Turns out it isn’t so.
In a stunningtwo-sentence letterto a federal appeals court, the Justice Department announced on Monday that it would now seek the invalidation of the entire Affordable Care Act — every last one of its thousands of provisions.
The irresponsibility of this new legal position is hard to overstate. It’s a shocking dereliction of the Justice Department’s duty, embraced by Republican and Democratic administrations alike, to defend acts of Congress if any plausible argument can be made in their defense.
Nor is the Affordable Care Act some minor statute that can be shoved aside without disruption. It is now part of the basic plumbing of the American health care system. It guarantees protections for people with pre-existing medical conditions. It expanded Medicaid to cover12.6 million more people, and it offers crucial protections to the156 million Americanswho get insurance through employers.
Beyond that, the law forces insurers to cover preventive care and contraception without charge; changed how hospitals and physicians bill for their services; requires fast-food restaurants to post calorie counts; cut hundreds of billions of dollars of Medicare spending; imposed hundreds of billions of dollars in taxes; and much, much more.
Unceremoniously ripping up the law would inflict untold harm on the health care system — and on all Americans who depend on it. Yet the Trump administration has now committed itself to doing just that.
The letter was submitted in a pending case, brought by a group of red states, in which a federal judge in Texas ruled that no part of the Affordable Care Act could stand. The judge reasoned that Congress created a constitutional problem when, in its big tax reform bill in 2017, it eliminated the financial penalty for going without insurance.
Because of that purported constitutional defect, the court held, the entire law had to fall. The ruling was indefensible: Legal scholarsacross the boardcriticized it as outrageous and predicted it would almost surely fall upon appeal.
Indeed, even the Trump administration couldn’t bring itself to argue that the entire law should be scrapped. It agreed there was a constitutional problem, but said that the right remedy was to keep most of the law in place.Only those partsrequiring private insurers to sell coverage at the same price to healthy and sick people alike — the protections for people with pre-existing conditions — would have to be struck.
That, too, was an outrageous position. It flouted the Justice Department’s duty to defend, a solemn duty, and one that goes to the heart of the rule of law. Without it, the sitting administration could pick which laws it wanted to defend in the courts and which it wanted to abandon. Laws could rise or fall based on nothing more than partisan disagreement. That’s inconsistent with a constitutional system that assigns to Congress — not the president — the power to legislate.
And so, at the confirmation hearing on his nomination to become attorney general, Mr. Barrsaidthat he would review the Justice Department’s position in the Texas lawsuit. Apparently he did just that — but instead of mounting a vigorous defense, he doubled down on killing Obamacare. It’s as if Mr. Barr said to his predecessor, Jeff Sessions: “You thought your position was crazy? Hold my beer.”
Does the administration really think that the very position it advanced just months ago is so untenable that it must now adopt one that is even more extreme?
The shift in legal position won’t make much of a difference in the lawsuit itself. Because a group of blue states has intervened, the appeals court will hear a full-throated defense of the law. Most observers expect the court to uphold the Affordable Care Act; if so, the Supreme Court may choose not to hear the case.
But the Trump administration has signaled loud and clear that its campaign against Obamacare is not over; that it will stop at nothing to achieve in court what it could not achieve in Congress; and that it doesn’t care how many people are hurt if the Affordable Care Act is undone.
It has also put health care back at the center of the political conversation. Republicans already took a beating on the issue in the fall midterm elections, and Democrats, whoreleased a bill in the Houseto strengthen the Affordable Care Act, want to keep running on it. They’ll be sure to remind voters of the Trump administration’s zealous commitment to taking away their health care.
Along the way, the Justice Department has trashed the duty to defend. That’s not to be taken lightly. The duty is a close cousin to the president’s constitutional duty to enforce the law. If the Justice Department really thinks that Obamacare is so blatantly unconstitutional that it can’t be defended, that implies that the president is violating the Constitution whenever he applies it.
It’s not hard to see that as an incipient justification for refusing to enforce any law that the president believes to be unconstitutional, however ridiculous or partisan that belief might be. Hopefully it doesn’t come to that. But the failure to defend the Affordable Care Act is an ominous sign to anyone who cares about the rule of law.
'How Will You Pay for It?' Bernie Sanders Tackles Key Question on Medicare for All
by Jake Johnson - Common Dreams - April 10, 2019
Sen. Bernie Sanders is not ducking the key question constantly posed to Medicare for All supporters by journalists, fellow members of Congress, and critics: "How will you pay for it?"
"'How are you going to pay for it?' That is the question that
bookends nearly every media conversation that takes place on Medicare
for All. The straightforward answer is, we already are." —Sen. Bernie Sanders' office
In a white paper (pdf) released Wednesday alongside the 2020 contender's updated and improved Medicare for All legislation,
Sanders' office outlined a number of possible funding mechanisms for
the comprehensive bill and detailed the enormous savings the U.S. would
reap by transitioning to single-payer.
"Every major industrialized nation on Earth has made healthcare a
right, provided universal coverage to all, and achieved far better
health outcomes in terms of life expectancy and infant mortality
rates—all while spending far less per capita than we do," the paper
states. "Please do not tell us that the United States of America, the
wealthiest nation in the history of the world, cannot do the same."
The paper lists a number of policy changes that could help raise revenue for Medicare for All, including:
A 70 percent top marginal tax rate on Americans earning over $10 million per year;
A 77 percent top tax rate on estates above $1 billion;
A tax on "extreme wealth";
A "fee on large financial institutions";
A "7.5 percent income-based premium paid by employers, exempting the
first $2 million in payroll to protect small businesses"; and
A four percent "income-based premium paid by employees, exempting the first $29,000 in income for a family of four."
While acknowledging its list is not exhaustive, Sanders' office
said the U.S. has a large "variety of options available to support a
Medicare for All, single-payer healthcare system."
"Under every single one of these options the average American family
will save thousands of dollars a year because it will no longer be
writing large checks to private health insurance companies," the
document says.
"The American people are increasingly clear. They want a healthcare
system which guarantees healthcare to all Americans as a right. They
want a healthcare system which will lower healthcare costs and save them
money." —Sen. Bernie Sanders
The white paper also emphasizes the massive savings American families
and the U.S. overall would reap by transitioning from the wasteful
for-profit system to Medicare for All, which would eliminate premiums,
deductibles, and co-pays.
"'How are you going to pay for it?' That is the question that
bookends nearly every media conversation that takes place on Medicare
for All," the paper states. "The straightforward answer is, we already
are."
"Unlike other government outlays—for example, a ship for the
Navy—Medicare for All does not represent any new spending at all," the
document continues. "Instead, it represents a rebalance of how our
current dollars are spent."
Under the for-profit status quo, Sanders' office points out, the U.S.
federal government is on track to spend $59.65 trillion on healthcare
between 2022 and 2031.
By contrast, according to two studies published last year, Medicare
for All would cost the U.S. significantly less while providing
comprehensive healthcare to all Americans.
"According to estimates from the conservative Mercatus Center,
under the Senate's Medicare for All legislation, [national healthcare]
expenditures will drop by approximately $2 trillion," the paper notes.
"Another study released by PERI
at the University of Massachusetts found that 'Medicare for All could
reduce total healthcare spending in the U.S. by nearly 10 percent,'
resulting in more than $5 trillion in savings."
Medicare for All would also save the U.S. money by slashing prescription drug costs, Sanders' office argued.
"If the U.S. joined the rest of the industrialized world and
negotiated with the pharmaceutical companies to lower prices, our
country could save up to $113 billion per year," the paper states.
The paper closes with a call for "vigorous debate" on the ideal path to funding Medicare for All.
As Vox's Sarah Kliff noted, the items offered by Sanders' paper "could no doubt be used to finance a national healthcare system."
"But eventually," Kliff added, "someone is going to have to pick which items on this list become law—and that's where things get tough."
"Unlike the Republican leadership in Congress which held no hearings
on their disastrous bill which would have thrown 32 million people off
of health insurance," Sanders' office concludes, "we will continue to
get the best ideas from economists, doctors, nurses, and ordinary
Americans to guarantee healthcare as a fundamental right."
The white paper was released as Sanders officially introduced his Medicare for All legislation with the support of 14 Democratic co-sponsors and more than 60 progressive advocacy groups.
"The American people are increasingly clear," Sanders said in a statement.
"They want a healthcare system which guarantees healthcare to all
Americans as a right. They want a healthcare system which will lower
healthcare costs and save them money. They want a healthcare system
which will guarantee them freedom of choice as to which doctor or
hospital they can go to."
"In other words," the Vermont senator added, "they want Medicare for All, and that's what we will deliver to them." https://www.commondreams.org/news/2019/04/10/how-will-you-pay-it-bernie-sanders-tackles-key-question-medicare-all?
'I Felt Americans Needed to Know': Insurance Industry Whistleblower Gives Glimpse of Effort to Crush Medicare for All
by Jake Johnson - Common Dreams - April 11, 2019
In an effort to inform the public about the corporate forces working
to crush Medicare for All, an employee at the insurance giant
UnitedHealthcare leaked a video of his boss bragging about the company's campaign to preserve America's for-profit healthcare system.
"I felt Americans needed to know exactly who it is that's fighting
against the idea that healthcare is a right, not a privilege." —whistleblower
"I felt Americans needed to know exactly who it is that's fighting
against the idea that healthcare is a right, not a privilege," the
anonymous whistleblower told the Washington Post's Jeff Stein.
During an employee town hall in February, Stein reported on Friday, UnitedHealthcare CEO Steve Nelson boasted about how much his company is doing to undermine Medicare for All, which is rapidly gaining support in Congress.
"One of the things you said: 'We're really quiet' or 'It seems like
we're quiet.' Um, we've done a lot more than you would think," Nelson
said. "We are advocating heavily and very involved in the conversation.
Part of it is trying to be thoughtful about how we enter in the
conversation, because there's a risk of seeming like it's self-serving."
According to the Post, which did not publish the video of
Nelson's remarks, the executive said his company "opposes Medicare for
All because it excludes the private sector, which he said does a better
job of delivering healthcare than the government, and said he doubted
how a single-payer system could be funded or effectively administered."
The UnitedHealth employee who leaked The Post
this video says: “I felt Americans needed to know exactly who it is
that’s fighting against the idea that healthcare is a right, not a
privilege."https://t.co/fQAXmVTmdf
Nelson's remarks were leaked just days after Sen. Bernie Sanders (I-Vt.), a 2020 presidential contender, unveiled his improved Medicare for All bill
with the support of 14 Democratic senators and over 60 progressive
organizations representing nurses, physicians, and consumer advocates.
Sanders called out insurance and pharmaceutical industry greed in a statement
following the introduction of his bill, which would virtually eliminate
the private insurance industry and provide comprehensive healthcare to
every American.
"When the people begin organizing against private insurance, the
lonely insurance executives turn to their only friends: the elected
officials beholden to their cash." —Tim Faust
"In my view, the current debate over Medicare for All really has
nothing to do with healthcare. It's all about greed and profiteering,"
said the Vermont senator. "It is about whether we maintain a
dysfunctional system which allows the top five health insurance
companies to make over $20 billion in profits last year."
On Friday, Sanders took to Twitter to send Nelson a message.
"When we are in the White House your greed is going to end," Sanders wrote.
Our message to Steve Nelson and UnitedHealthcare
is simple: When we are in the White House your greed is going to end. We
will end the disgrace of millions of people being denied health care
while a single company earns $226 billion and its CEO makes $7.5 million
in compensation. https://t.co/OafOIT92H9
UnitedHealth Group, the parent company of United Healthcare, raked in
around $17 billion in profits and "spent about $8 million on lobbying
efforts" in 2018, Stein reported.
UnitedHealthcare's fight against single-payer, Stein noted, comes
"amid a broader push from the health insurance industry to prevent
legislation to enact Medicare for All from getting off the ground,
including by trying to direct Democrats toward more centrist efforts and
reject plans that would effectively legislate many of the companies out
of existence."
"[A]bout half a dozen representatives of lobbying firms said they had
pushed for meetings with Democrats over single-payer and other proposed
government expansions of healthcare," according to Stein.
In a statement to the Post, Medicare for All campaigner and
policy expert Tim Faust said, "When the people begin organizing against
private insurance, the lonely insurance executives turn to their only
friends: the elected officials beholden to their cash."
One of the industry-backed groups leading the fight against Medicare
for All is the Partnership for America's Health Care Future, which is comprised of major pharmaceutical and insurance interests.
The Partnership launched a six-figure ad campaign against Medicare for All earlier this year, warning the popular proposal "would cause massive disruption to the current healthcare system."
After the Partnership launched its first digital ad against Medicare for All in January, Wendell Potter—an insurance industry executive-turned-whistleblower—said, "It's almost impressive how many lies they're able to fit into such a short clip."
Watch Potter's breakdown of the Partnership's ad: https://www.commondreams.org/news/2019/04/12/i-felt-americans-needed-know-insurance-industry-whistleblower-gives-glimpse-effort?
Republican Health Care Lying Syndrome
by Paul Krugman - NYT - April 1, 2019
There are three kinds of lies: lies, damned lies and Republican claims about health care.
O.K., it’s not news that politicians make misleading claims, some more than others. According to a running tally kept by Daniel Dale of The Toronto Star, as of Monday morning, Donald Trump had said 4,682 false things as president.
But
G.O.P. health care claims are special, in several ways. First, they’re
outright, clearly intentional lies — not dubious assertions or
misstatements that could be attributed to ignorance or misunderstanding.
Second, they’re repetitive: Rather than making a wide variety of false
claims, Republicans keep telling the same few lies, over and over.
Third, they keep doing this even though the public long ago stopped
believing anything they say on the subject.
This syndrome demands
an explanation, and I’ll get there eventually. Before I do, however,
let’s document the things that make G.O.P. health care lies unique. [For an even deeper look at what’s on Paul Krugman’s mind, sign up for his weekly newsletter.]
First,
as I said, I’m not talking about mere dubious claims. When Trump
officials insisted that the 2017 tax cut would lead to a decade of
miraculous growth, their claim made no sense in terms of the underlying economics,
and it flew in the face of decades of evidence. But it was a
prediction, not a statement of fact, and it’s conceivable (barely) that
Trump’s people actually believed it.
But when Mick Mulvaney, the acting White House chief of staff, went on TV Sunday to declare that “every single plan” Trump has put forward “covered pre-existing conditions,” that was just a lie.
Here’s what the Congressional Budget Office said
in its assessment of the Republicans’ American Health Care Act, which
would have caused 23 million to lose coverage, and would have passed if
John McCain hadn’t voted “No”: “People who are less healthy (including
those with pre-existing or newly acquired medical conditions) would
ultimately be unable to purchase comprehensive nongroup health insurance
at premiums comparable to those under current law, if they could
purchase it at all.”
But Mulvaney’s pre-existing conditions lie,
along with his lie about nobody losing coverage if the lawsuit against
Obamacare succeeds, was normal by G.O.P. standards. Which brings me to
the second reason this particular form of lying is exceptional:
Republicans just keep telling the same lies, over and over. Again and
again they have promised to maintain coverage and protect pre-existing
conditions — then offered plans that would cause tens of millions to
lose health insurance, with the worst impact on those already suffering
from health problems.
The funny thing — which is my third point —
is that almost nobody seems to believe these lies. On the eve of last
year’s midterm elections, the public trusted Democrats over Republicans
to protect Americans with pre-existing conditions by 58 percent to 26
percent. A margin this big tells us that even Trump supporters knew
their man was lying on this issue.
So what’s behind the persistence of R.H.L.S. — Republican health care lying syndrome?
Well,
public opinion here is clear: Americans want everyone to have access to
health care. There isn’t even that much of a partisan divide: An overwhelming majority of Republicans don’t believe insurance companies should be allowed to deny coverage or charge more to those with pre-existing conditions.
This public near-unanimity is one reason Medicare is so popular. Getting older — and thus joining a group with much higher average health costs than the rest of the population — is, after all, the ultimate pre-existing condition.
But there are only two ways to cover people with pre-existing conditions, and both are anathema to conservative ideology.
One is to have taxpayers pay the bills directly, which is what Medicare does.
The
other combines regulation and subsidies. Insurance companies must be
prohibited from discriminating based on medical history — a prohibition
that must include preventing them from issuing bare-bones policies that
will appeal only to those in good health — but that won’t do the job by
itself. Healthy people must also be induced to sign up, to provide a
good risk pool, which means subsidizing premiums for those with lower
incomes and, preferably although not totally necessary, imposing a
penalty on those without insurance.
If the second option sounds
familiar, it should. It’s what countries like the Netherlands and
Switzerland do; it’s also a description of, you guessed it, Obamacare.
But
Republicans cannot admit that the only way to protect pre-existing
conditions is to emulate Democratic policies. The party of Eisenhower,
or even the party of Nixon, might have been able to do such a thing, but
the party of Fox News cannot.
Nor, however, do Republicans dare
admit that they have no interest in providing protection that a vast
majority of voters demands. So they just keep lying.
You may, by
the way, have heard talk about G.O.P. members of Congress opposed to
Trump’s new health care push. But they share his goals; they’re just
questioning his timing. The whole party still wants to take away your
health care. It just hopes to get through the next election before you
find out. https://www.nytimes.com/2019/04/01/opinion/republicans-health-care.html?smid=nytcore-ios-share
Don’t Make Health Care a Purity Test
by Paul Krugman - NYT - March 21, 2019
We’re now in the silly season of the Democratic primary — a
season that, I worry, may last all the way to the nomination. There are
many honorable exceptions, but an awful lot of reporting seems to be
third order — not about the candidates, let alone their policy
proposals, but about pundits’ views about voters’ views of candidates’
electability. It’s a discussion in which essentially nobody has any idea
what he or she is talking about.
Meanwhile, however, there are
some real continuing policy debates. They’re not mainly about goals:
Whoever the Democrats nominate will profess allegiance to a progressive
agenda aimed at reducing inequality, strengthening the social safety net
and taking action on climate change. But there are some big differences
about how to achieve those goals.
And the starkest divide involves health care. Almost surely, the eventual platform will advocate “Medicare for TK.” But what word is eventually chosen to replace the placeholder “TK,”
and more important, what that means in terms of actual policy, will be
crucial both for the general election and for what comes after if
Democrats win.
On one side, there’s “Medicare for All,” which has
come to mean the Bernie Sanders position: replacing the entire existing
U.S. health insurance system with a Medicare-type program in which the
government pays most medical bills directly.
On the other side, there’s “Medicare for America,” originally a proposal from the Center for American Progress, now embodied in legislation.
While none of the announced Democratic candidates has endorsed this
proposal yet, it’s a good guess that most of them will come around to
something similar. [For an even deeper look at what’s on Paul Krugman’s mind, sign up for his weekly newsletter.]
The
big difference from a Sanders-type plan is that people would be allowed
to keep private coverage if they chose — but they or their employers
would also have the option of buying into an enhanced version of
Medicare, with substantial subsidies for lower- and middle-income
families.
The most important thing you need to know about these rival plans is that both of them would do the job.
Many
people realize, I think, that we’re the only advanced country that
doesn’t guarantee essential health care to its legal residents. My guess
is that fewer realize that nations achieve that goal in a variety of
ways — and they all work.
Every two years the Commonwealth Fund provides an invaluable survey
of major nations’ health care systems. America always comes in last; in
the latest edition, the three leaders are Britain, Australia and the
Netherlands.
What’s remarkable about those
top three is that they have radically different systems. Britain has
true socialized medicine — direct government provision of health care.
Australia has single-payer — it’s basically Bernie down under. But the
Dutch rely on private insurance companies
— heavily regulated, with lots of subsidies, but looking more like a
better-funded version of Obamacare than like Medicare for All. And the
Netherlands actually tops the Commonwealth Fund rankings.
So which
system should Democrats advocate? The answer, I’d argue, is the system
we’re most likely actually to create — the one that will play best in
the general election, and is then most likely to pass Congress if the
Democrat wins.
And there’s one big fact on the ground that any realistic health strategy has to deal with: 156 million Americans
— almost half the population — currently receive health insurance
through their employers. And most of these people are fairly satisfied
with their coverage.
A Medicare for All plan would in effect say
to these people, “We’re going to take away your current plan, but trust
us, the replacement will be better. And we’re going to impose a bunch of
new taxes to pay for all this, but trust us, it will be less than you
and your employer currently pay in premiums.”
The thing is, both
of these claims might well be true! A simple, single-payer system would
probably have lower overall costs than a hybrid system that preserves
some forms of private coverage.
But even if optimistic claims
about Medicare for All are true, will people believe them? And even if
most people do, if a significant minority of voters doesn’t trust the
promises of single-payer advocates, that could easily either doom
Democrats in the general election or at least make it impossible to get
their plan through Congress.
To me, then, Medicare for America —
which lets people keep employment-based insurance — looks like a much
better bet for actually getting universal coverage than Medicare for
All. But I could be wrong! And it’s fine to spend the next few months
arguing the issue.
What won’t be fine will
be if activists make a no-private-insurance position a litmus test,
declaring that anyone advocating a more incrementalist approach is no
true progressive, or maybe a corrupt shill for the medical/industrial
complex. As you might guess, my concerns aren’t drawn out of thin air;
they’re things I’m already hearing.
So Democrats should try to
make this a real debate, one about the best strategy for achieving a
shared goal. Can they manage that? I guess we’ll find out. https://www.nytimes.com/2019/03/21/opinion/medicare-for-all-democrats.html?smid=nytcore-ios-share
Opinion | Elissa Ely: Measuring medical care in 20-minute doses - The Boston Globe
by Elissa Ely - Boston Globe - April 12 2019
Consider 20 minutes: a middling amount of time,
not as ample as 47 minutes or as brief as 6, but an interval that seems
long enough to wave at someone over the fence post and maybe hang out a
bit.
Twenty minutes is also long enough to greet a patient in the
waiting room, walk them down the hall, take their weight, fill out
their group-home paperwork, check their refills, see if the Care Plan is
updated in the Electronic Medical Record, and send an e-mail to Central
Scheduling with a follow-up date. It’s probably enough time to inquire
about sleep, appetite, exercise, voices, and bowel function. “How’s your
mood these days?” 20 minutes asks — but when the answer comes, it
doesn’t have time to listen hard. Someone else is already waiting by the
fence post.
Twenty minutes is not long enough to find out what
the greatest worry in life is at the moment, or which TV show offers
respite (bless those Kardashians). It can’t stop to admire how someone
continues to cope with decades of illness — and, if her son happens to
be recovering from an overdose, it’s not long enough to learn the
details. A patient terrified of an upcoming medical procedure will have
to hold onto that thought.
Twenty minutes doesn’t stop for crisis, and even stopping for sorrow
can become a luxury. It’s good for productivity requirements, bad for
relationships.
With all this high efficiency, patients — who are in no position to
argue — may not feel eager to rush back for another 20 minutes.
Caretakers are in no position to argue either. We have this in common
(though naturally, there is not enough time to talk about it).
A number of months ago, a man came in. He was in the depressed phase
of a cycle, barely able to rise off the sofa. We discussed a medication
change, which took all our time. I asked if he would come back sooner
than usual.
“For what?” he said.
“Just to talk,” I said.
He looked surprised.
“Really?” he said. “I didn’t know psychiatrists did that.’’ Elissa Ely is a psychiatrist. https://www.bostonglobe.com/opinion/2019/04/12/measuring-medical-care-minute-doses/9QAhkd96XxRojj6do0MOGP/story.html?et_rid=1744895461&s_campaign=todayinopinion:newsletter
Patients express frustration over surprise medical bills - The Boston Globe
By Liz Kowalczyk - Boston Globe - April 13, 2019
Cheryle Reidel knows a thing or two about surprise medical bills.
There was the $6,000 for a cancer biopsy in 2012. Several years later,
an anesthesiologist and a nurse anesthetist billed her $2,600 for
another procedure.
This year, it happened again: Reidel underwent a
colonoscopy at Norwood Hospital — which is fully covered by her
insurance plan — only to discover that the anesthesiologist who worked
there was not. The bill: $2,490.
What happened after Reidel, 64, received these unexpected medical
charges illustrates one of the most frustrating and unpredictable
aspects of the health care system: It was only after dozens of phone
calls and numerous letters to insurance companies and the providers that
she got these bills
dismissed. Other patients have not been so lucky.
Reidel was one of more than 25 readers who wrote to the Globe after the newspaper published a story last month about out-of-network billing, expressing frustration with unexpected charges.
The 10 top local news stories from metro Boston and around New England delivered daily.
“The patient should not be on the hook for spending hours and hours
digging through paperwork, printing out documents, and contacting the
insurance company, contacting the anesthesiologists, contacting the
hospital,’’ Reidel said. “That’s ridiculous. I work a full-time job.’’
Chloe Nasser’s parents have been relentlessly fighting such bills.
Last summer, her doctor, who is affiliated with Brigham and Women’s
Hospital, ordered routine blood work — at a lab in the same office. She
was astonished to get a $701.89 bill a month later because the lab was
not in her insurance network.
The family is also contesting a much
larger out-of-network bill for a colonoscopy Nasser had at the Brigham,
said her mother, Kathleen Wynn.
Surprise out-of-network medical bills occur when a hospital uses
anesthesiologists, radiologists, ambulance companies, emergency medicine
doctors, or other providers that are not covered by a patient’s
insurance network. Often, providers do not inform patients in advance.
The practice is under growing scrutiny nationwide. A new analysis
shows these charges, also called balance billing, may be more common in
Massachusetts than previously believed.
A study by the nonprofit
Health Care Cost Institute found that 15 percent of 9,041 in-network
hospital admissions in Massachusetts in 2016 included an out-of-network
bill from a professional who worked there — the 11th-highest rate in the
country.
David Seltz, executive director of the Massachusetts
Health Policy Commission, a watchdog group, cautioned that the study
only examined medical claims from large national insurers.
Massachusetts-based insurers tend to have more providers in their
networks, so there is less chance for a patient to be hit with a
surprise medical bill.
Still, the new information “reinforces the
need and urgency for the [state] to take action to address this issue
and help protect patients,’’ Seltz said.
The Globe reported in
March that about 115 patients filed complaints about surprise medical
bills in 2017 and 2018 with Massachusetts Attorney General Maura
Healey’s office. Readers responded to the article quickly and
passionately.
One theme was clear: Patients usually just paid bills that ran in the
hundreds of dollars because they were either too busy or too sick to
fight over relatively small amounts; however, others with large balances
were relentless in challenging the charges. Many readers held hospitals
responsible for using out-of-network doctors.
The Globe reviewed bills to verify readers’ complaints.
A few examples: ■ Nancy Welsh took her diabetic daughter to
Emerson Hospital’s emergency department last July because she wasn’t
eating or drinking. Doctors started intravenous fluids and called
Armstrong Ambulance Service to transfer her to Boston Children’s
Hospital.
Several weeks later, the family received a bill for more
than $3,000. Armstrong, it turns out, was not covered by their Aetna
insurance plan. After eight phone calls, four e-mails, and a registered
letter, Aetna reimbursed Welsh in February.
“A lot of people would have given up,’’ she said. “The more they stalled, the angrier I got.’’
But
Welsh wondered why staff at the Concord hospital did not warn her in
advance. Emerson spokeswoman Leah Lesser said there are so many
different and ever-changing insurance companies and plans that it is
often not possible to determine a patient’s coverage in an emergency.
“We encourage patients, before they need care, to learn what is covered by their insurance plans,’’ Lesser said in a statement. ■ Jonathan Scott, 61, was diagnosed with
advanced cancer in 2016. Scott’s oncologist and surgeon at Beth Israel
Deaconess Medical Center were covered by his Tufts Health Plan network,
as was the hospital, he said. Another surgeon — apparently not covered —
was assigned to implant a tiny catheter above Scott’s heart through
which he would get chemotherapy.
Weeks later, he received a bill for $1,198.
“I
couldn’t eat or walk and I was having to deal with the insurance
company,’’ Scott said. Tufts eventually agreed to waive the charges, he
said.
Hospital spokeswoman Jennifer Kritz said she could not
comment on Scott’s case because of patient privacy rules but said
patients generally need prior approval from their insurance companies
for procedures.
Patients have been receiving these unexpected
bills for years. Doctors often blame insurers for the problem, saying
the large national companies don’t pay enough for them to join their
networks. Meanwhile, insurers argue that doctors prefer to remain
out-of-network because that allows them to charge inflated rates, rather
than accept a negotiated fee.
A number of states
have passed laws regulating out-of-network billing. After failing to
pass consumer projections last year, Massachusetts legislators plan to
reconsider similar measures this year.
Hospital officials often
say the problem is between insurers and doctors’ groups. State laws
typically include a way for the two sides to reach fair payment rates.
But Frederick Isasi,
executive director of the nonprofit Families USA, said hospitals share
the blame.
“They are selecting their providers,’’ said Isasi, who
recently testified before Congress on the issue. “They have a
responsibility to make sure they are in-network.’’
Reidel, a sales analyst for a medical supply company, agrees.
Her first two surprise bills involved care she received at Sturdy Memorial Hospital in Attleboro, which was in her insurance plan’s network, she said.
Amy
Pfeffer, Sturdy’s chief financial officer, said the hospital strongly
encourages all providers to join the same networks as the hospital but
does not require it. Mandating it, she said, might force doctors to
accept smaller payments from insurers that do not cover their costs.
“That would tie their hands,’’ she said.
After
receiving the $2,490 bill from Ether Anesthesia of Massachusetts
following her colonoscopy at Norwood Hospital last year, Reidel left a
message for the hospital’s chief executive. Reidel said two weeks later,
Norwood’s Chief Financial Officer Elizabeth Ganem told her the charges
were resolved.
When asked why Norwood Hospital allows
out-of-network anesthesiologists to work there, spokeswoman Lisa
Tarabelli said in an e-mail that the “hospital is in the process of
bringing the provider in-network.’’
Chloe Nasser’s family is
unsure whether they will succeed in their battle over large
out-of-network medical bills for medical care at Brigham and Women’s
Hospital.
Ethan Slavin, a spokesman for Aetna, her insurer at the
time, said many Aetna plans include the Brigham in their network. But
not Nasser’s particular plan; her Brigham doctor was covered, but the
hospital itself was not. And that is where her doctor sent some lab work
and where he sent her for a colonoscopy. Wynn, Nasser’s mother, said no
one mentioned this possibility.
The Brigham said it is improving
its educational materials for patients to better explain the medical
bills they might face. That information is expected to be ready in May. https://www.bostonglobe.com/metro/2019/04/13/patients-express-frustration-over-surprise-medical-bills/dKHCsHYVfF35QtKidoV75K/story.html?et_rid=1744895461&s_campaign=todaysheadlines:newsletter
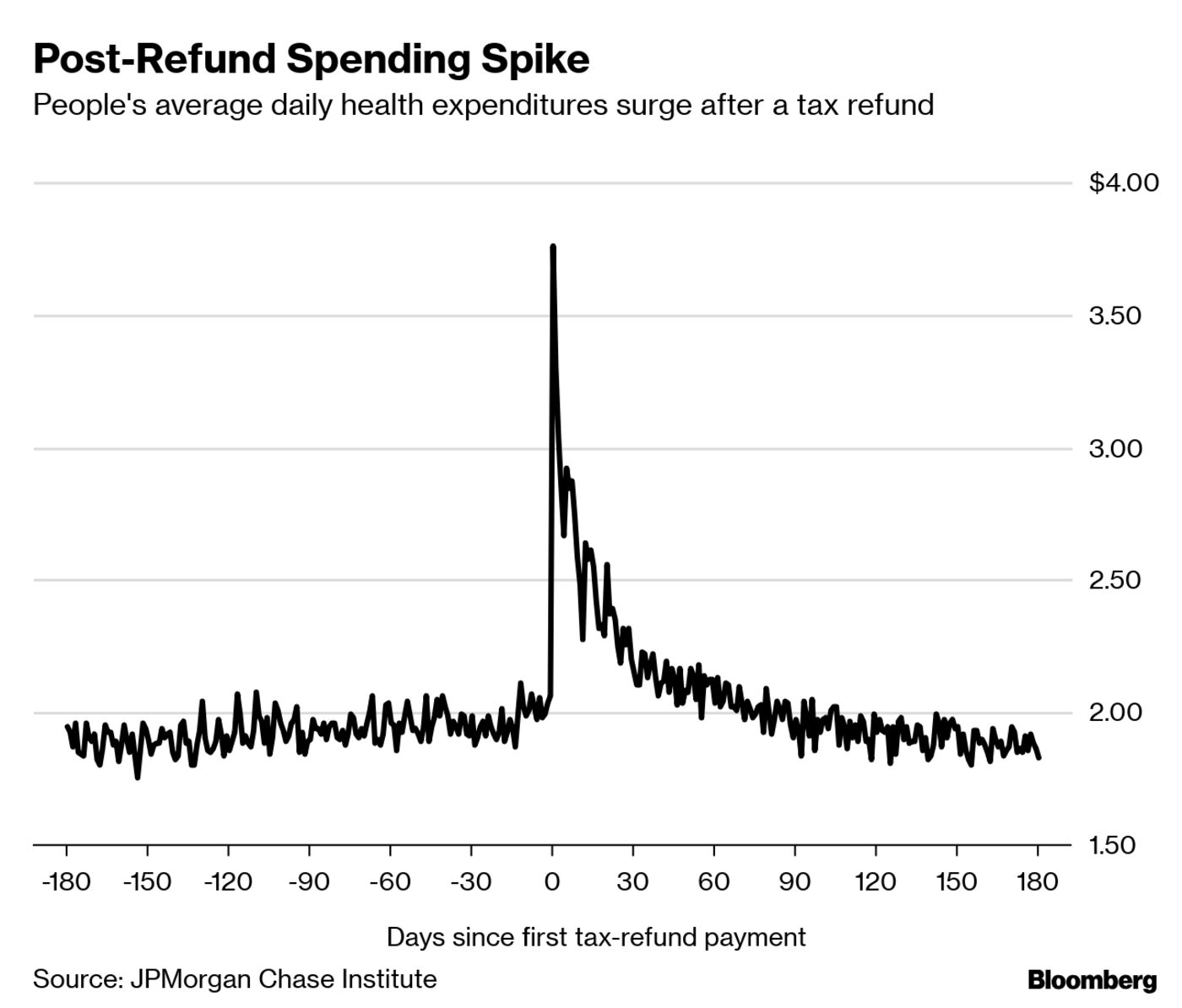
Americans Are Delaying Health Care Until Tax Refunds Arrive
Out-of-pocket medical spending jumps once the money hits people’s bank accounts.
by John Tozzi - Bloomberg News - April 12, 2109
When Hayden Myer made an eye doctor’s appointment for the end of
April, he told the clinic that he might not show up for the visit if his
tax refund didn’t arrive in time.
The 27-year-old, who says his vision is bad enough that he
avoids driving at night, has been wearing a four-year-old pair of
glasses since he ran out of contact lenses last summer. He’s expecting
about $265 from his refund.
Myer and many other Americans rely on getting money back at
tax time to pay for important health needs. It’s a result of thin
household savings colliding with rising medical prices and high-deductible insurance plans that expose them to greater health expenses.
“I’ve
never been able to use my return for anything that is a leisure or a
pleasure,” said Myer, who earns about $40,000 a year running a
peer-support line for a mental-health nonprofit in Richmond, Virginia.
The
federal deadline for people to file income taxes is April 15.
Out-of-pocket spending on health care jumps about 60 percent in the week
after people get their refunds, according to an analysis
of account data published last year by the JPMorgan Chase Institute, a
research group that draws on the bank’s data. The bulk of that money is
spent during face-to-face encounters at clinics, hospitals or other
medical providers.
That suggests people aren’t merely using refunds to pay down
old debts; they’re waiting until they have cash in hand to get treated.
“It
was surprising, and I’d go so far as to say alarming,” said Fiona
Greig, director of consumer research at the JPMorgan Chase Institute.
“Those are visits that would have taken place three weeks earlier, had
the tax refund arrived three weeks earlier.”
Refunds trigger about a 10 percent increase in the number of
people making in-person health-care payments on weekdays, according to
the group’s research. Other research from the institute has shown that
refunds are also frequently followed by increased cash withdrawals,
credit card payments and spending on durable goods.
Tax refunds — the difference between the money withheld from workers’ paychecks and the taxes they actually owe — are the biggest single payment many households receive all year. The average federal refund taxpayers received this spring was $2,873, according to IRS data on filings as of March 29.
More
than 1 in 3 working-age Americans skipped a doctors’ visit or medical
test, or didn’t fill a prescription, because of the cost last year,
according to a recent survey by the Commonwealth Fund, a nonprofit health-research foundation.
Myer,
who has insurance, has been forgoing weekly injections for low
testosterone, getting them only once a month or less. “That prescription
is also just sky-high,” he said, costing about $75 per visit until he
reaches his health plan’s deductible.
The medical costs add to a
pile of student loans, credit-card debt and payments on his Nissan
Rogue. He recently moved back in with his father after he couldn’t
afford a rent increase. He also owes money to a psychiatrist who charges
a sliding-scale fee. Getting a new prescription for his vision is
Myer’s priority, though.
Spring Surge
Dentists and
physicians’ offices accounted for the greatest share of in-person
health payments that followed tax refunds, the JPMorgan Chase
Institute’s report showed. Mark Vitale, a dentist in Edison, New Jersey,
said refunds always bring a surge of patients.
“Year after year, what patients will say to me is, ‘Let’s
just wait until April 1 or May 1 when I get my tax refund,’” he said.
Vitale has practiced for 35 years, and over time, he said, “the dollar
has gotten tighter.’’
Three people who booked significant dental
procedures like implants or crowns around the beginning of April cited
their tax refunds, he said. They’re typically employed, middle-class
people. Sometimes they’ve delayed dental work for years.
The research group analyzed data from millions of Chase bank
accounts, as well as credit and debit cards, looking for patterns in the
movements of money.
The granular picture of how cash flow affects
people’s ability to get medical care reveals problems that clinicians,
health plans, employers and financial companies ought to grapple with,
said Greig.
Doctors need to talk to patients about how to
prioritize care if they can’t pay for it. That conversation now happens
“in a very incomplete way” with finance staff, rather than clinicians,
she said. Employers and health plans should understand that trying to
lower spending by pushing more expenses onto households could backfire
if they delay care.
“Health problems don’t age well,” Greig said. https://www.bloomberg.com/news/articles/2019-04-12/what-to-spend-your-tax-refund-on-how-about-the-doctor
I have been reading your posts regularly which is specially for health, medicine and body care .I need to say that you are doing a fantastic work. Please keep it up the great work. leg pain
I would be grateful if you continue with the quality of what we are doing now with your blog.I really enjoyed it
ReplyDeletetravel and medical insurance
I have been reading your posts regularly which is specially for health, medicine and body care .I need to say that you are doing a fantastic work. Please keep it up the great work.
ReplyDeleteleg pain